
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Hassan Yassin Lumbe*, Arnold Landolin Wella, Rickson Geoffrey Bahati, Bulebhe Gerald Magesa, Adrian Saveli Maketta
Corresponding Author: Hassan Yassin Lumbe, Songea Regional Referral Hospital, P.O. Box 5, Songea, Tanzania.
Received: December 27, 2025 ; Revised: December 29, 2025 ; Accepted: January 2, 2026 ; Available Online: January 8, 2026
Citation: Lumbe HY, Wella AL, Bahati RG, Magesa BG & Maketta AS. (2026) Perforated Peptic Ulcer Disease in East Africa: A Systematic Review of Epidemiology, Management Challenges, and Outcomes. J BioMed Adv Clin Res, 3(1): 1-5.
Copyrights: ©2026 Lumbe HY, Wella AL, Bahati RG, Magesa BG & Maketta AS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Background: Perforated Peptic Ulcer Disease (PPUD) remains a life-threatening surgical emergency globally. In East Africa, its epidemiology, clinical presentation, and management outcomes are shaped by distinct regional factors including high rates of Helicobacter pylori infection, delayed presentation, and systemic healthcare challenges. Despite advances in surgical care, PPUD continues to pose significant public health and clinical burdens in this resource-limited region.
Objective: To synthesize existing evidence on the epidemiology, clinical management, and outcomes of PPUD in East Africa, and to identify region-specific challenges and opportunities for improving care.
Methods: A systematic search of PubMed, African Journals Online (AJOL), Google Scholar, and WHO Global Index Medicus was conducted up to March 2025, following PRISMA 2020 guidelines. Studies reporting on PPUD incidence, etiology, management, and outcomes in East African countries were included. Two reviewers independently screened, extracted, and appraised data.
Results: Of 127 identified records, 22 met the inclusion criteria. PPUD in East Africa predominantly affects young to middle-aged males, with a male-to-female ratio of approximately 3:1. H. pylori infection is implicated in 60–80% of cases, with NSAID use and smoking as significant co-factors. Delayed presentation is common, with the mean duration from symptom onset to hospital admission ranging from 2 to 5 days. Pneumoperitoneum on erect abdominal X-ray remains the primary diagnostic tool, though its sensitivity is limited in late presentations. Surgical management is almost exclusively open laparotomy with Graham’s omental patch repair. Postoperative mortality rates range from 5% to 15%, driven mainly by sepsis, delayed intervention, and limited critical care resources. Challenges include diagnostic delays, shortage of surgical personnel, lack of laparoscopic equipment, and limited access to postoperative ICU care.
Conclusion: PPUD in East Africa is a frequent surgical emergency associated with significant morbidity and mortality, largely attributable to systemic and resource-related delays. Strengthening early diagnosis at primary care levels, expanding surgical training and capacity, and integrating H. pylori screening and eradication into national health programs are critical steps toward reducing the burden of this preventable disease.
Keywords: Perforated peptic ulcer; East Africa; surgical emergency; Helicobacter pylori; Graham’s patch; resource-limited settings; Tanzania; Kenya; Uganda; morbidity; mortality
INTRODUCTION
Peptic ulcer disease (PUD) and its complications represent a significant cause of acute surgical admission globally. Perforation, the most severe complication, carries a high risk of mortality if not managed promptly [1]. In high-income countries, the incidence of PPUD has declined markedly due to widespread use of proton pump inhibitors (PPIs), effective H. pylori eradication, and reduced smoking. However, in East Africa, PPUD remains a common and devastating surgical emergency, reflecting persistent challenges in primary healthcare access, diagnostic capacity, and timely surgical intervention [2].
The clinical presentation of PPUD in East Africa is often atypical or advanced, due to initial misdiagnosis as malaria, typhoid, or gastroenteritis in primary care settings [3]. This diagnostic anchoring, compounded by socioeconomic barriers to healthcare access, results in prolonged patient delays before definitive surgical management. Additionally, the high prevalence of H. pylori infection exceeding 80% in some adult populations—creates a large at-risk pool for ulcer development and perforation [4].
Management is further challenged by limited surgical infrastructure, shortage of trained personnel, and scarce critical care support, especially in rural and regional hospitals [5]. Despite these constraints, open surgical repair remains a life-saving procedure with good outcomes when performed expediently [6].
This systematic review aims to consolidate current evidence on the epidemiology, clinical management, and outcomes of PPUD in East Africa. By highlighting region-specific patterns and systemic gaps, this review seeks to inform clinical practice, surgical training, and public health policy aimed at reducing the morbidity and mortality associated with this preventable surgical catastrophe.
METHODOLOGY
Protocol and Guidelines
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [7].
Search Strategy
We searched PubMed/MEDLINE, African Journals Online (AJOL), WHO Global Index Medicus, and Google Scholar for studies published between January 2000 and March 2025. Search terms included: (“perforated peptic ulcer” OR “peptic ulcer perforation”) AND (“East Africa” OR “Tanzania” OR “Kenya” OR “Uganda” OR “Rwanda” OR “Burundi” OR “Ethiopia”) AND (“epidemiology” OR “management” OR “outcomes” OR “mortality”).
Eligibility Criteria
We included observational studies, case series (≥10 patients), and comparative studies conducted in East Africa that reported on incidence, etiology, clinical features, management, or outcomes of PPUD. Studies in languages other than English were excluded if no translation was available.
Screening and Data Extraction
Two reviewers independently screened titles, abstracts, and full texts. Disagreements were resolved by consensus. Data on study design, setting, sample size, patient demographics, etiology, diagnostic methods, treatment, complications, and mortality were extracted.
Quality Appraisal
Quality appraisal using the Joanna Briggs Institute (JBI) tools indicated that most included studies were of moderate methodological quality [8].
RESULTS
Study Selection
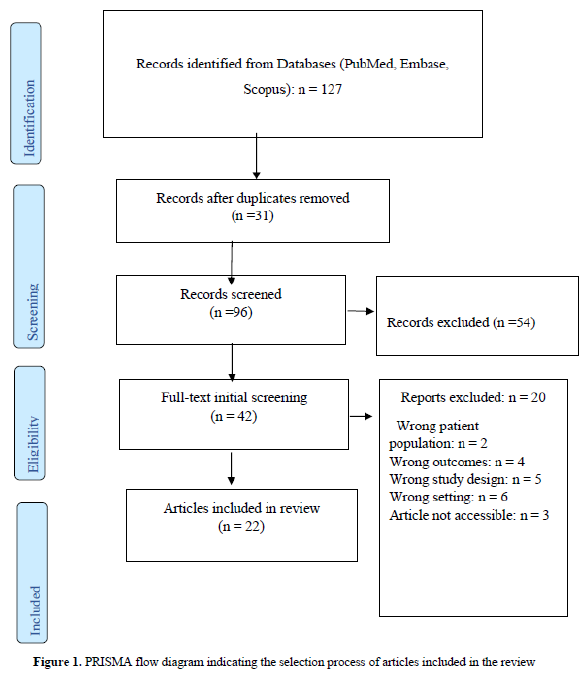
The initial search yielded 127 records. After removing duplicates (n=31) and screening titles/abstracts, 42 full-text articles were assessed. Twenty-two studies met inclusion criteria (Figure 1).
Epidemiology and Demographics
PPUD in East Africa shows a male predominance (M:F ≈ 3:1), with a mean age of 35–45 years younger than reported in high-income settings [9]. Incidence rates are difficult to ascertain due to underreporting, but PPUD constitutes 5–15% of all acute surgical admissions in major referral hospitals [10]. Seasonal variations have been noted, with higher incidence during rainy months, possibly linked to increased rates of gastrointestinal infections and NSAID use for febrile illnesses [11].
Etiology and Risk Factors
Clinical Presentation and Diagnosis
Patients typically present late, with symptom duration averaging 48–72 hours before hospital arrival [3]. Common misdiagnoses at primary care level include malaria, typhoid, and acute gastroenteritis. Classic signs of peritonitis (rigidity, guarding, rebound tenderness) are present in over 80% of cases on admission [9]. Erect abdominal X-ray confirms pneumoperitoneum in 70–85% of cases [12]. Ultrasound and CT are rarely used due to cost and limited availability.
Management and Surgical Approaches
All studies reported open surgical management as the standard of care. Graham’s omental patch repair was performed in >90% of cases [6]. Peritoneal lavage with warm saline (3–6 litres) was uniformly described. Laparoscopic repair is virtually unavailable in public sector hospitals. Postoperative care includes intravenous antibiotics (commonly ceftriaxone and metronidazole), PPIs, and analgesics. ICU admission is rare, even for critically ill patients, due to bed shortages [5].
Outcomes and Complications
Postoperative complications occur in 20–30% of cases, most commonly surgical site infection, intra-abdominal abscess, and sepsis [13]. Mortality rates range from 5% to 15%, with higher rates in elderly patients, those with delayed presentation (>48 hours), and in hospitals without onsite surgical specialists [1, 14]. Survivors generally have good long-term outcomes, though recurrence rates are understudied.
Systemic Challenges
The management of this condition faces multifaceted systemic barriers that impede effective care across the continuum. Key challenges begin with diagnostic delays, often stemming from initial misdiagnosis in primary care and patient initial reliance on traditional healers [15]. Furthermore, surgical workforce shortages mean many district hospitals lack specialist surgeons [16]. Even when diagnosis occurs, limited infrastructure including a lack of laparoscopic equipment, insufficient ICU beds, and unreliable oxygen supply constrains treatment options [17]. Financial constraints pose another significant hurdle, as out-of-pocket costs for surgery and medications severely limit patient access [18]. Finally, the pathway of care remains fragmented beyond the operating room, characterized by inadequate postoperative follow-up and poor patient adherence to essential therapies such as H. pylori eradication [19].

DISCUSSION
This review highlights that PPUD in East Africa is not only a surgical disease but a marker of systemic healthcare gaps [20, 21]. The young age of presentation and strong association with H. pylori point to opportunities for primary and secondary prevention that are currently underutilized [21].
The near-universal use of open Graham’s patch repair demonstrates the resilience of this low-cost, effective technique in resource-limited settings [22]. However, the absence of laparoscopic options reflects a significant technological gap. While laparoscopy may not be immediately scalable, training in laparoscopic repair for PPUD should be incorporated into surgical residency programs in the region to build future capacity.
Mortality remains unacceptably high, driven largely by delays rather than surgical technique [23]. Interventions must therefore focus on the pre-hospital and pre-operative phases: improving diagnostic accuracy at primary care level through clinical decision tools, ensuring prompt referral, and strengthening ambulance and emergency transport systems.
From a public health perspective, integrating H. pylori screening and eradication into national non-communicable disease or digestive health programs could significantly reduce the incidence of PUD and its complications [25]. Similarly, regulating over-the-counter NSAID sales and promoting community awareness of “red flag” abdominal symptoms may reduce late presentations [25].
Future research should prioritize the establishment of prospective multicenter registries to better define the disease incidence and patient outcomes, providing a crucial epidemiological foundation. This should be complemented by cost-effectiveness analyses of H. pylori “test-and-treat” strategies within high-prevalence regions to guide resource allocation [29]. Furthermore, implementation studies are needed to evaluate the task-shifting of diagnostic ultrasound to trained non-physician clinicians in rural hospitals, aiming to overcome workforce shortages. Concurrently, the development and validation of a practical risk score for use in primary care settings could help in early identification and intervention [30].
Strengths and Limitations
This review is the first to systematically synthesize data on PPUD specific to East Africa, providing a focused regional perspective. Limitations include heterogeneity in study design and data reporting, publication bias toward urban referral centers, and the lack of population-based incidence data.
CONCLUSION
Perforated peptic ulcer disease remains a frequent, life-threatening emergency in East Africa, where it affects a younger population and is driven by high H. pylori prevalence and healthcare access delays. While Graham’s omental patch repair is a robust and life-saving intervention, outcomes are heavily influenced by systems failures before the patient reaches the operating table.
A multipronged strategy is essential: strengthening primary care diagnostic accuracy, expanding surgical workforce and infrastructure, investing in emergency referral systems, and implementing preventive H. pylori management. By addressing these challenges, East African health systems can significantly reduce the morbidity, mortality, and economic burden of this preventable surgical disease.
FUNDING STATEMENT
The authors received no specific funding for this work.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
ACKNOWLEDGEMENTS
The authors would like to express their sincere gratitude to the administration of Songea Regional Referral Hospital for their support. We are also thankful to the librarians and staff at the various institutions who assisted with accessing the full-text articles necessary for this review. We acknowledge the authors and publishers of all studies included in this systematic review, whose work made this synthesis possible.

No Files Found




Internationally Accepted
Share Your Publication :