
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Komal Razzaq*, Umair Arif, Iqra Tahir, Touseef-ur-Rehman, Asima Liaqat, Kaiynat Shafique, and Hafiz Muhammad Almas Sabir
Corresponding Author: Komal Razzaq, Physiotherapist, Female OPD In charge, The University of Faisalabad, Canal Road, Faisal Town, Pakistan
Received: February 02, 2022 ; Revised: March 27, 2022 ; Accepted: April 10, 2022 ; Available Online: May 1, 2022
Citation: Razzaq K, Arif U, Tahir I, ur-Rehman T, Liaqat A, et al. (2022) A Comparative Study to Analyze the Effect of Planter Fascia Stretch and Heel Pad with Moist Heat in the Patients of Planterfascitis. J Ageing Rehab Res, 1(1): 1-6.
Copyrights: ©2022 Razzaq K, Arif U, Tahir I, ur-Rehman T, Liaqat A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Abstract
Background: This study investigated the effect of planter fascia stretch and heel pad with moist heat in the patients of planterfascitis among subjects aged 20-40. Planter fascia is a thickened fibrous sheet of connective tissue which begins from medial tubercle on undersurface of calcaneus and fans out joining to the metatarsophalangeal joints plates to form longitudinal foot arch. Manual active stretching or passive stretching of planter fascia and Achilles’s tendon are effective treatment option for patient with planter fasciitis.
Aims and Objectives: objectives of this study were to see the effect of planter fascia stretch and heel pad with moist heat in the patients of planterfascitis.
Material and Methodology: This study was quasi experimental study. It took samples by convenient method from 80 subjects among Faisalabad private hospitals community. The study was completed in the duration of 3 months. Data was conducted through convenient sampling from Faisalabad private hospitals. This study explored the effect of planter fascia stretch and heel pad with moist heat on subjects aging 20-40 years old. Subjects were allocated to group A (n=40) and group B (n=40). Group A received treatment as planter fascia stretch and group B received treatment as heel pad with moist heat. Follow up were taken after 4 weeks in 3-month duration study.
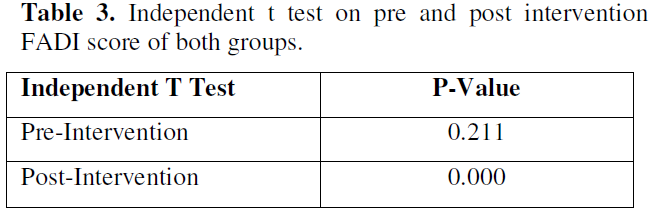
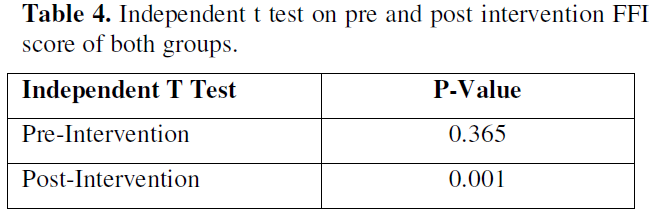
Results: Statistical Analysis Data were analyzed using SPSS version 23.0. Intragroup comparison of differences between pre and post intervention scores of FFI and FADI was analyzed using independent T Test. The results were considered statistically significant if p values were less than 0.05.). No statistically significant difference was observed in pre intervention score between the groups on FADI (p = 0.211) and FFI (p = 0.365), but, statistically significant difference was observed between all the groups on post intervention score with respect to FADI (p=0.000) and FFI (p=.001) as analyzed by independent t test.
Conclusion: After applying the entire treatments and measuring pre and post value it conducted that planter fascia stretch has more significant effect on planterfascitis than heel pad with moist heat.
Keywords: Planterfascitis, Planter fascia stretch, Heel pad with moist heat
INTRODUCTION
Planter fascia is a thickened fibrous sheet of connective tissue which begins from medial tubercle on undersurface of calcaneus and fans out joining to the metatarsophalangeal joints plates to form longitudinal foot arch. Planter fasciitis is a degenerative syndrome of planter fascia due to repeated trauma as its origin on the calcaneus. Planter fasciitis is very significant cause of pain of heel on slightly inferior side. Discomfort and pain related with condition can have considerable effect on physical mobility. Etiology of planter fasciitis is multifactorial in nature. Increase in weight, anatomical changes improper foot wear, bad biomechanics, work related issues and over activities are major contributing factors in developing the condition of planter fasciitis [1].
Sometimes it becomes severe and take month or even year to resolve and become challenging for clinicians. Other names for planter fasciitis include calcaneodynia, sub calcaneal pain, runners’ heel, heel spur syndrome and painful heel syndrome. Decreased ankle dorsiflexion, weight bearing for long period, pes planus and sudden weight gain are the major risk factors for planter fasciitis. Signs and Symptoms are localized tenderness of calcaneus bone at anteromedial aspect, stiffness of Achilles tendon, pain increased by passive dorsiflexion of toes after standing on tip of toes. Significant pain after performing heavy activities or after weight bearing exercise. The exact presentation of planter fasciitis is pain on the sole foot at inferior border of heel. Patient feels severe pain after taken few steps in morning [2].
Most options for treatment are available which show different level of efficiency. Some conservatives’ options for treatment like rest, avoiding aggressive or heavy activity, strengthening and stretching exercises, night splinting and orthotics. Other options to treat planter fasciitis are anti-inflammatory agents, electrotherapy (Ultrasonic shock wave therapy), steroidal injection and surgery. Time to resolve this issue varies from almost 6 to 18 months. Sometimes may be longer which may become challenge for both patient and clinician. Many experts think identification, diagnosis and treatment in early stage of disease brings better recovery in comparatively short period of time [3].
Splinting and walking casts help the patient of planter fasciitis to keep his foot in neutral position overnight. It reduces the pressure on heel at heel strike. Silicon insole is a non- invasive treatment option which add comfort and provide soothing effect to heal as it absorbs about 50% of shock during walking. Some studies suggests that silicon insole provide good relief to patient with planter fasciitis that the custom-made orthotics and stretching exercises do alone and it is one of most effective treatment options for increasing functional status and decreasing pain in patient with planter fasciitis pain [4].
Manual active stretching or passive stretching of planter fascia and achillea tendon are effective treatment option for patient with planter fasciitis. There are many studies have been tested the efficiency of planter fascia stretch and Achilles’ tendon stretch with positive result. Some studies also evaluated the effectiveness of combined treatment including ultrasound or radial shock wave therapy and stretching exercises the result of the same studies suggested that combined treatment of stretching of gastrocnemius and ultrasound and planter fascia being are as effective as radial shock wave therapy and stretching of planter fascia and gastrocnemius. Some studies showed the result for combined treatment of calcaneal taping and planter fascia stretch [5].
Stretching of calf muscle is also very effective in patient of planter fascia according to same studies. Only some studies that suggest the superior of calf stretch over planter fascia stretch or planter fascia stretch over calf stretch. Some studies also compared the superiority of planter stretch over stretch of tendon Achilles and the result revealed the stretch of planter fascia is relatively more effective than tendon Achilles stretch in patient of planter fascia. Combination of both stretch (planter fascia stretch and calf stretch) are very effective in resolving the issue, restoring the normal range of motion and decreasing the pressure from stiff and tight planter fascia. But there is no study has identified the independent efficiency of these exercises [6].
Some studies show that non-steroidal anti-inflammatory drugs in decreasing pain and reducing the inflammation of planter fascia, but the efficiency of these drugs in patient with chronic issue still remain obscure. Some researches show the positive result with moist heat while treating patient with planter fascia but the effectiveness of moist heat in isolation remains uncertain. Moist heat shows better result when used in combination with other modalities like heel pad [7,8].
To our knowledge, there will be no literature of study that has compared and assess independent efficiency of two commonly used treatment modalities like heel pad with hot fomentation and stretching exercises of planter fascia. So, the objective of recent study is to evaluate the response of planter fasciitis patient to different treatment options when given separately that may support to establish a conclusive treatment strategy for managing patient with planter fasciitis [3,9].
MATERIAL AND METHODOLOGY
This study was quasi experimental study. It took samples by convenient method from 80 subjects among Faisalabad private hospitals community. The study was completed in the duration of 3 months. Data was conducted through convenient sampling from Faisalabad private hospitals. It used to see the effect of planter stretch and heel pad with moist heat in the patients of planter fasciitis. This study explored the effect of planter fascia stretch and heel pad with moist heat on subjects aging 20-40 years old. Subjects were allocated to group A (n=40) and group B (n=40). Group A received treatment as planter fascia stretch and group B received treatment as heel pad with moist heat. Follow up were taken after 4 weeks in 3 months duration study.
Inclusion criteria
Exclusion criteria
It was a quasi-experimental study in which 80 members of both genders are equally divided into two groups of group A and group B with 40, 40 members in which group A received treatment as heel pad with moist heat while group B received treatment as planter fascia stretch. A treatment given to both groups for 4 days per week and complete session was of 3 months duration. Both treatments were given under supervision. Follow up was taken after 4 weeks of each month.
Statistical analysis
Statistical Analysis Data were analyzed using SPSS version 23.0. Intragroup comparison of differences between pre and post intervention scores of FFI and FADI was analyzed using independent T Test. The results were considered statistically significant if p values were less than 0.05.
RESULTS
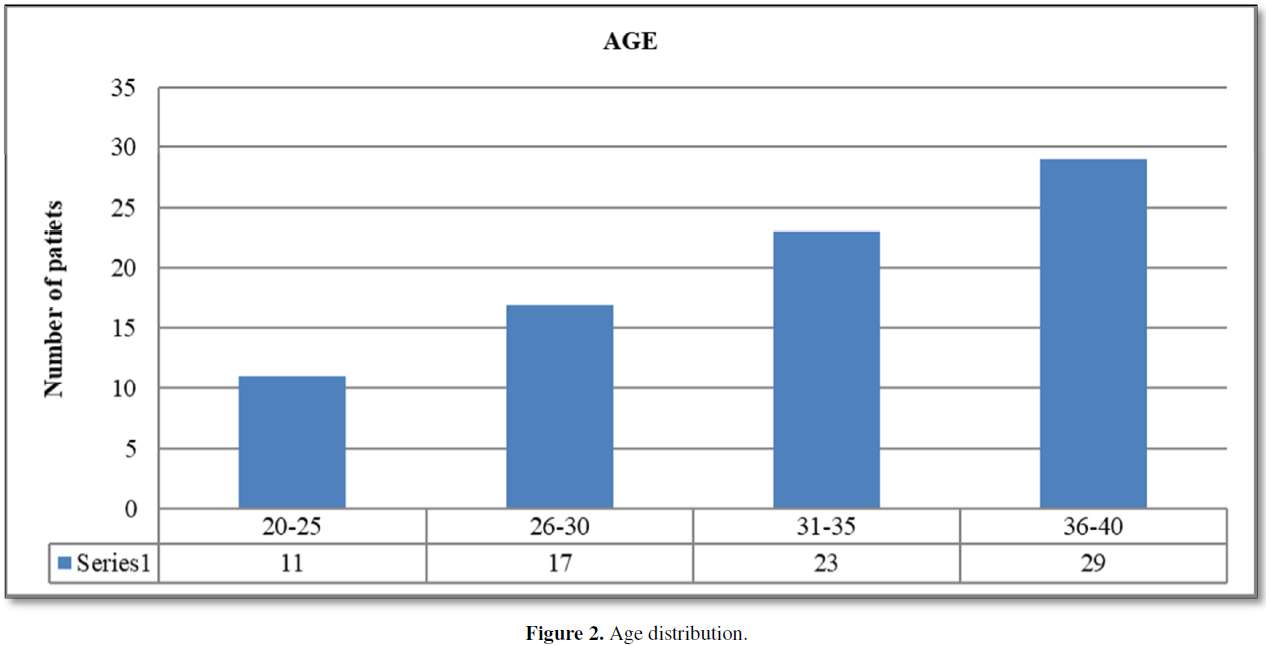
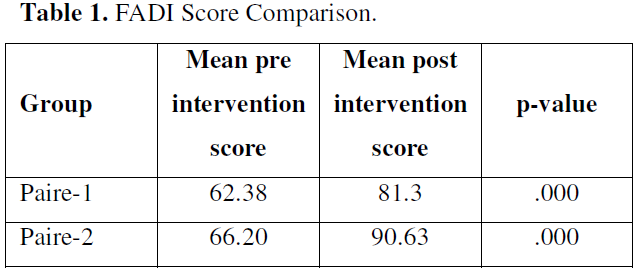
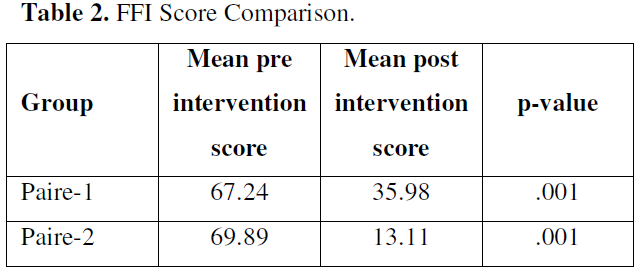
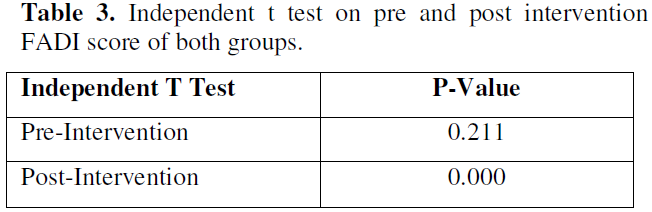
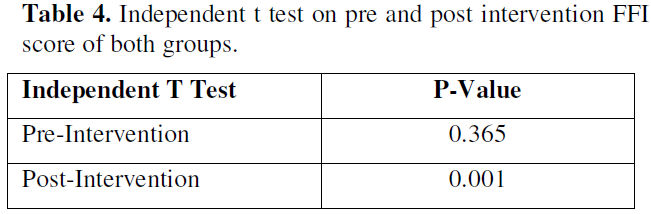
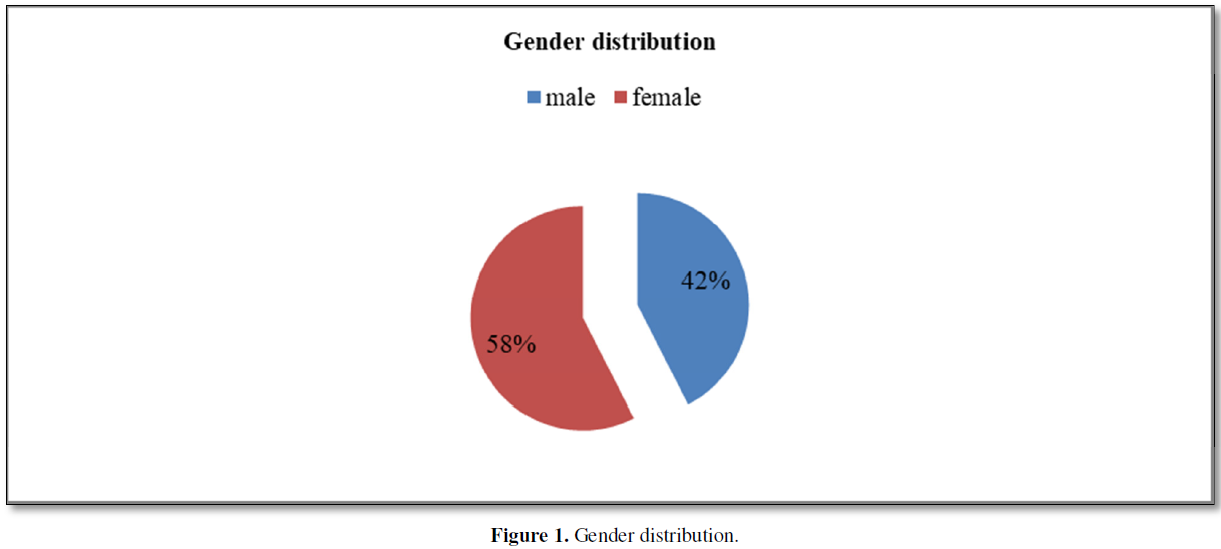
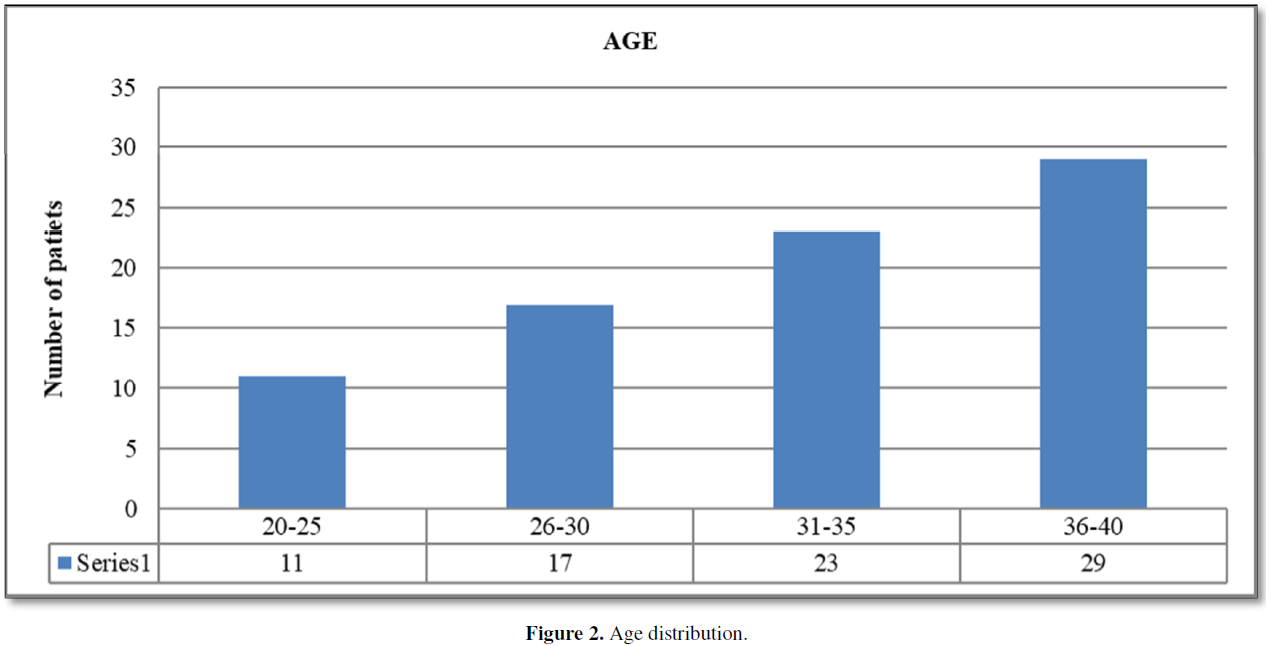
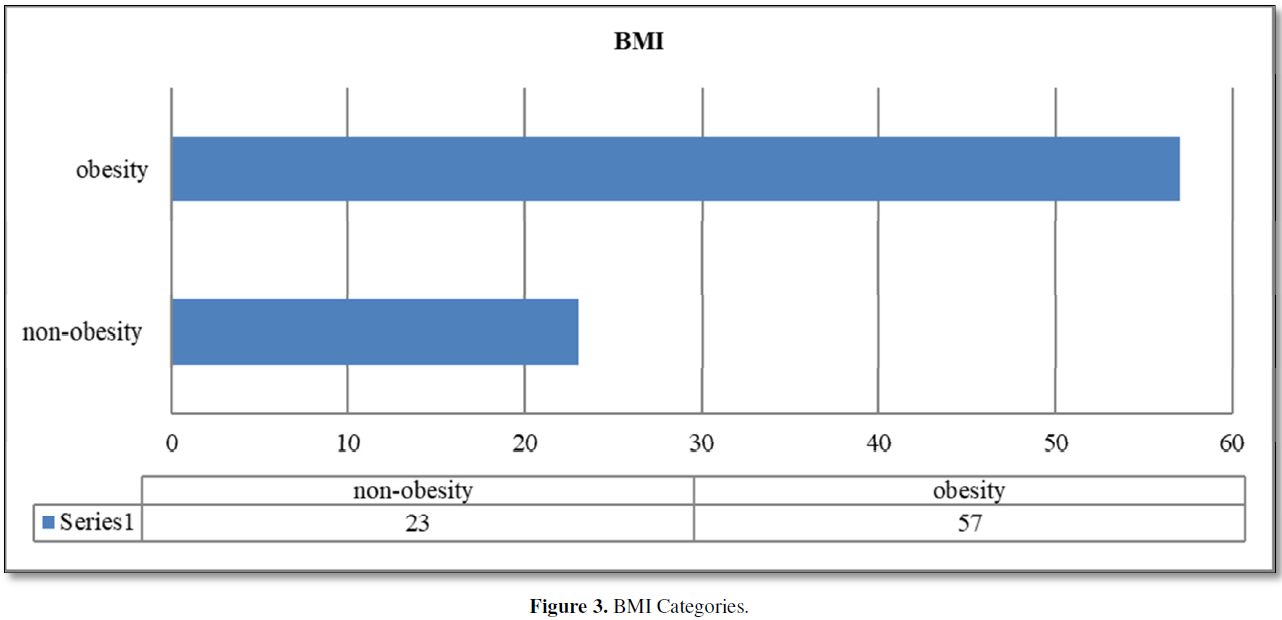
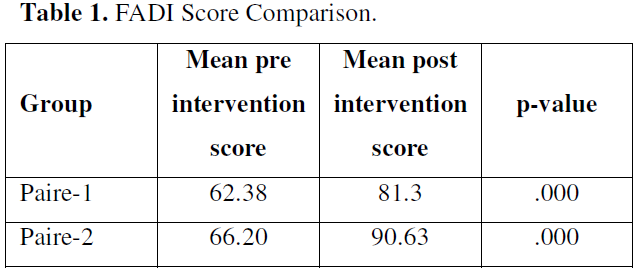
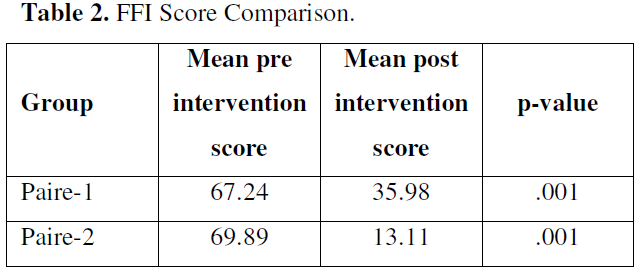
Total 80 patients were included in our study. 40 were randomly allocated to group A and 40 were allocated to group B. Out of 80 patients 34(42%) were male and 46(58%) were female (Figure 1). Out of 80 patients 11 were lie in age group of 20-25, 17 were lie in age group of 26-30, 23 were lie in age group of 31-35 and 29 were lies in age group of 36-40. Average age was 32.61±3.94 (Figure 2). Out 80 patients 57 were overweight and 23 were not overweight. Average BMI was 27.32±4.82 (Figure 3). Significant difference was founded on FADI score on both pairs with p-value 0.000 (Table 1). Significant difference was founded on FFI score on both pairs with p-value 0.000 (Table 2). No statistically significant difference was observed in pre intervention score between the groups on FADI (p = 0.211) and FFI (p = 0.365), but, statistically significant difference was observed between all the groups on post intervention score with respect to FADI (p=0.000) and FFI (p=.001) as analyzed by independent t test (Tables 3 & 4).
CONCLUSION
After applying the entire treatments and measuring pre and post value it conducted that planter fascia stretch has more significant effect on planterfascitis than heel pad with moist heat.
DISCUSSION
Plantar fasciitis is a debilitating condition that causes pain on the inferior aspect of the foot, particularly when taking the first few steps in the morning [2]. Most options for treatment are available which show different level of efficiency. Some conservative’s options for treatment like rest, avoiding aggressive or heavy activity, strengthening and stretching exercises, night splinting and orthotics [2]. To our knowledge, there will be no literature of study that has compared and assess independent efficiency of two commonly used treatment modalities like heel pad with hot fomentation and stretching exercises of planter fascia. So, the objective of recent study is to evaluate the response of planter fasciitis patient to different treatment options when given separately that may support to establish a conclusive treatment strategy for managing patient with planter fasciitis. In our study total 80 patients were included and randomly allocated to group A and B. Out of 80 patients 34(42%) were male and 46(58%) were female. In the present study, we have observed the predominance of female patients over the male patients. This is in line with the study of Davis et al., 74 female patients and 31 male patients with plantar fasciitis were included [2,11], and in another study by Yucel [12] heel pain was found to be more common in the female population (76.6 percent in females vs. 23.3 percent in males. This disparity between male and female ratios in our sample may be attributed to factors such as long periods of standing, more frequent use of overweight or high heel boots, and the habit of barefoot walking among women. Out of 80 patients, in our study ,11 was lie in age group of 20-25, 17 were lie in age group of 26-30, 23 were lie in age group of 31-35 and 29 were lies in age group of 36-40. This shows that the prevalence of planter fasciitis increases with the age. These results are in accordance with the study of Matheson [13]. They discovered that younger athletes had a lower incidence of plantar fasciitis (2.5%) than older athletes (6.6%) in a retrospective study of 1407 patients from an outpatient sports medicine clinic [14].
Results of the present study depict that the plantar fascia stretching group showed more reduction in pain and improvement in activities as compared to the silicone heel pad plus hot fomentation group as observed from mean difference. Significant difference was founded on FADI score on both pairs with p-value 0.000. Significant difference was founded on FFI score on both pairs with p-value 0.000. No statistically significant difference was observed in pre intervention score between the groups on FADI (p = 0.211) and FFI (p = 0.365), but, statistically significant difference was observed between all the groups on post intervention score with respect to FADI (p=0.000) and FFI (p=.001). Prefer [15] compared three prefabricated shoe inserts (a rubber heel cup, a felt insert, and a silicone heel pad) with Achilles’ tendon and plantar fascia stretching against stretching alone on 236 patients in a randomized controlled study. Just 190 patients completed the 8-week follow-up, but the silicone insert group had a higher response rate than the stretching-only group (p=0.019). Although the silicone insert group improved better on FFI than the stretching alone group, there was no statistically significant difference (p=0.54) [16]. Another research by Yucel [12]. found that after using full-length insoles, the condition of 80% of patients improved, with a statistically significant difference in mean pain ratings at p
Davis [18] published a retrospective review, conducted on 105 patients, 89 percent of patients were shown to improve significantly with non-operative treatment which included rest, NSAIDs, Achilles’ tendon and plantar fascia stretching exercises, and heel cushions. Stretching exercises, on the other hand, were found to be the most effective therapy for plantar fasciitis in their research [14]. For a better result, various writers have recommended the use of stretching exercises in the treatment of plantar fasciitis. The effect of plantar fascia and calf stretching exercises was seen in 101 patients suffering from chronic plantar fasciitis in phase one of a clinical trial for 8 weeks of treatment, according to Digiovanni [19]. The treatment plan also included prefabricated soft insoles and a 3-week course of celecoxib, in addition to the stretching exercises. After 8 weeks, patients in the plantar fascia stretching community showed significant improvement on the FFI pain score in terms of worst pain; p=0.02 and first steps in the morning; p=0.006, but no significant improvement was shown when all of the FFI components were compared. After 8 weeks of care, patients in the calf stretch group were advised to perform plantar fascia stretching exercises [14]. At 2 years of follow-up in phase two of the clinical trial both groups progressed significantly in terms of pain and visual analogue scale scores from baseline on FFI score (p0.0001). As a result, these findings indicate that plantar fascia stretching exercises offer greater symptom relief in cases of plantar fasciitis [14].
REFERENCES
No Files Found




Internationally Accepted
Share Your Publication :