
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Lysandre Bourguignon*, Louis-Philippe Baraby, Jean-Sébastien Audet and Frederick Aardema#
Corresponding Author: Lysandre Bourguignon and Frederick Aardema, Centre de recherche de lInstitut Universitaire en santé mentale de Montréal, 7331 Hochelaga, Montréal, Québec, H1N 3V2, Canada.
Received: February 24, 2026 ; Revised: March 03, 2026 ; Accepted: March 05, 2026 ; Available Online: March 12, 2026
Citation: Bourguignon L, Baraby LP, Audet JS & Aardema F. (2026) The Identification of an Absorption Factor in the Dissociative Experiences Scale in a Clinical Sample with Obsessive-Compulsive Disorder. J Psychol Psychiatry Res, 3(1): 1-8.
Copyrights: ©2026 Bourguignon L, Baraby LP, Audet JS & Aardema F. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Recent evidence suggests that dissociative absorption (DA) may be a clinically relevant tendency in Obsessive-Compulsive Disorder (OCD). Utilizing the Dissociative Experiences Scale (DES), Soffer-Dudek et al. (2015) identified a purified DA factor that was meaningful to OC symptoms in a non-clinical population. The current study aimed to replicate these findings in an OCD sample. Hypotheses were: (1) DA would be a unique factor in a three-factor model of the DES; (2) DA would significantly predict OCD symptoms; (3) DA scores would be significantly higher for OCD participants than for controls. Using confirmatory factor analyses, a three-factor model was not supported, while the DA factor alone performed outstandingly. DA significantly predicted OCD symptoms. Results suggest that DA is relevant to OCD symptomatology, but may not be characteristic of OCD in general. The eight-item DA factor is well-suited for further investigations into the role of DA in OCD as a stand-alone questionnaire.
Keywords: Dissociative Experiences Scale; dissociation; absorption; obsessive-compulsive disorder; self-report; confirmatory factor analysis.
INTRODUCTION
Obsessive-Compulsive Disorder (OCD) is a highly disabling psychiatric disorder characterized by recurrent intrusive thoughts (obsessions) and repetitive behaviors or mental acts (compulsions) aimed at reducing distress or preventing feared consequences (American Psychiatric Association, 2013; Overduin & Furnham, 2012). Increasing evidence suggests that dissociative processes may play a role in OCD symptomatology, particularly in relation to checking compulsions (Aardema & Wu, 2011; Paradisis, Aardema, & Wu, 2015; Soffer-Dudek, Lassri, Soffer-Dudek, & Shahar, 2015)
Despite growing interest, the scope and definition of dissociation remain debated. While some conceptualize dissociation as a continuum ranging from normal to pathological experiences, others argue for distinct dissociative entities (Holmes et al., 2005). Diagnostic systems also differ in their conceptualization of dissociation (American Psychiatric Association, 2013; World Health Organization, 1992). The DSM-5 defines dissociation as a disruption in the normal integration of consciousness, whereas some authors emphasize that dissociation becomes pathological only when it interferes with access to information or self-awareness (Leavitt, 2001).
More recently, Soffer-Dudek (2014) proposed that a specific dissociative process, dissociative absorption (DA), may be particularly relevant to OCD. Absorption refers to the tendency to become fully immersed in mental experiences, resulting in narrowed attention and reduced awareness of the external environment (Tellegen & Atkinson, 1974; Putnam, 1997). During such states, individuals may act automatically while vividly imagining scenarios, which can blur the distinction between imagination and reality (Soffer-Dudek et al., 2017).
Although DA is not recognized as a distinct dissociative disorder and is not inherently pathological (Kihlstrom, 2005), it closely overlaps with the concept of inferential confusion, a cognitive process central to OCD in which imagined possibilities are mistaken for real probabilities (O'Connor & Aardema, 2003). Through inferential confusion, individuals with OCD may develop obsessions that lack grounding in sensory information and become increasingly absorbed in imagined scenarios, leading to experiences resembling dissociation (Aardema & O'Connor, 2007).
Dissociation is commonly assessed using the Dissociative Experiences Scale (DES-II; Carlson & Putnam, 1993), which includes absorption, amnesia, and depersonalization/ derealization factors. However, the factor structure of the DES remains controversial. While some studies support multi-factor models, others suggest that the scale primarily measures a general dissociative trait (Bernstein, Ellason, Ross, & Vanderlinden, 2001; Zingrone & Alvarado, 2001). Concerns have also been raised regarding the specificity of the DA factor, as many absorption items show substantial overlap with general dissociation (Soffer-Dudek et al., 2015).
Addressing these issues, Soffer-Dudek et al. (2015) identified a purified eight-item DA factor and demonstrated that DA was a stronger and more specific predictor of OCD symptoms than general psychopathology, and the only dissociative construct to longitudinally predict OCD symptoms. These findings suggest that DA may represent a clinically meaningful dissociative tendency in OCD.
However, most studies examining the structure of the DES have relied on non-clinical samples. Although analogue samples are informative, findings may not generalize to clinical populations, where symptom dynamics are often more complex (Aardema et al., 2017; Melli, Aardema, and Moulding., 2016). Moreover, the specificity of DA to OCD, relative to other disorders such as anxiety or depression, remains largely unexplored. Therefore, further investigation of the factor structure and clinical relevance of DA in individuals with OCD is warranted.
Aims and hypotheses of the present study
The current study aimed to investigate the underlying structure of the DES by attempting to replicate the findings from Soffer-Dudek et al. (2015) in an OCD clinical sample. It was hypothesized that: (1) DA is a unique dissociative factor within a three-factor structure of the DES; (2) the purified DA factor would significantly predict symptoms of OCD; and (3) those with OCD would score significantly higher on DA than clinical controls (mixed anxiety disorder (AD) and depression disorder (DD) group) and non-clinical controls (NCC).
METHOD
Procedure
Participants were recruited at the Obsessive-Compulsive Research Laboratory of the Centre de recherche de l’Institut universitaire en santé mentale de Montréal. The study received ethics approval from the local ethics board, and all participants provided written informed consent. Clinical participants were recruited through professional and self-referrals and were diagnosed using the Structured Clinical Interview for DSM-IV (SCID-I; First et al., 1995) by an independent evaluator. Exclusion criteria included substance abuse, suicidal ideation, schizophrenia, bipolar disorder, or organic disorder. All participants completed the questionnaires at a single time point.
The non-clinical control (NCC) group was recruited through local newspaper advertisements and received CAD $20 compensation. A trained graduate student conducted a telephone screening for psychopathology using a structured SCID-I–based questionnaire (Kirouac et al., 2006). Participants with any indication of psychopathology were excluded, and eligible participants received the questionnaire battery by mail.
Participants
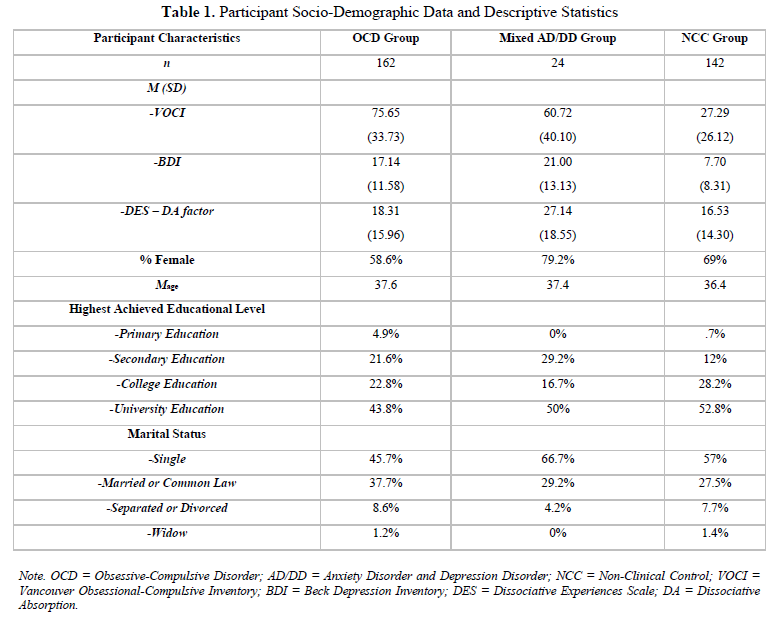
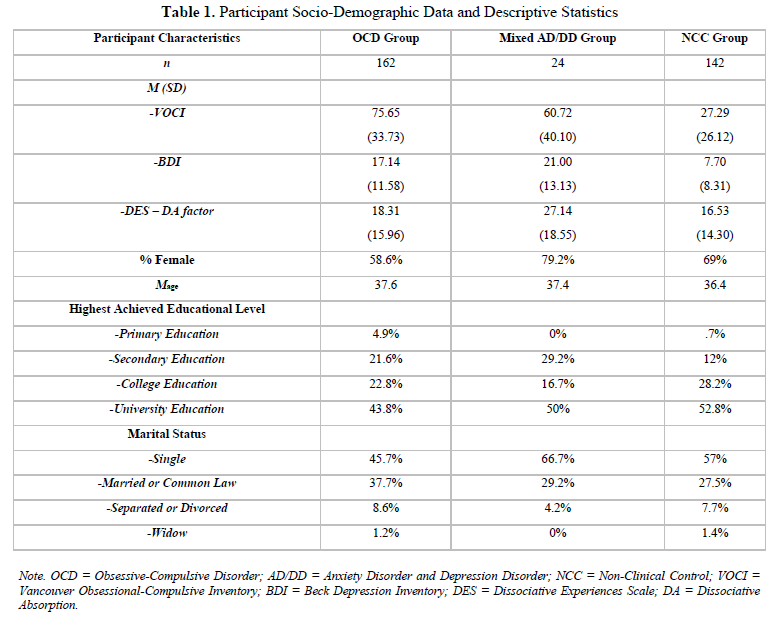
Socio-demographic data for all participants are presented in Table 1. There were three groups of participants in the study: an OCD group (n = 162), a mixed AD/DD group (n = 24) and a NCC group (n = 142). In addition to the SCID‐I, participants in the OCD group were administered the clinician version of the Yale–Brown Obsessive–Compulsive Scale (Y‐BOCS; Goodman, Price, Rasmussen, Mazure, Delgado, et al., 1989; Goodman, Price, Rasmussen, Mazure, Fleischmann, et al., 1989) to assess OCD severity and nature of their OCD; this revealed a mean score of 25.84 (SD = 6.76), indicating moderate-to-severe levels of OCD. Participants in the AD/DD clinical comparison group were diagnosed with either a primary anxiety disorder (AD) or a depressive disorder (DD).
Measures
Dissociative Experiences Scale. The Dissociative Experiences Scale (DES-II; Carlson & Putnam, 1993) is a 28-item self-report measure (11-point scale, 0 to 100, increasing by increments of 10) that assesses the frequency of dissociation in both clinical and non-clinical populations. The global score is obtained by adding up the 28 item scores and dividing by 28, which yields an overall score ranging from 0 to 100. Three underlying factors have previously been identified yielding three subscales: absorption/imaginative involvement, dissociative amnesia and depersonalization/derealization. This measure possesses high reliability properties (α = .93-95; Frischholz, Braun, Sachs, & Hopkins, 1990; Van IJzendoorn & Schuengel, 1996).
Beck Depression Inventory – II. The Beck Depression Inventory – II (BDI-II; Beck, Steer, & Brown, 1996) is a 21-item instrument elaborated to measure the severity of depressive symptoms experienced by participants during the 2 weeks prior to completion. Frequently used by researchers, this questionnaire has shown to be highly reliable and a valid measure of depressive symptoms (α = .92–.93; Beck et al., 1996).
Vancouver Obsessional-Compulsive Inventory. The Vancouver Obsessional-Compulsive Inventory (VOCI; Thordarson et al., 2004) is a 55-item self-report questionnaire designed to assess OCD symptoms, including obsessions, compulsions, avoidance behaviors, and associated personality characteristics. It comprises six analytically derived subscales: obsessions, checking, contamination, just right, indecisiveness, and hoarding (Aardema et al., 2013; Thordarson et al., 2004). Items are rated on a five-point Likert scale ranging from 0 (“not at all”) to 4 (“very much”) (e.g., “I am often very upset by my unwanted impulses to harm other people”).
The VOCI has demonstrated excellent internal consistency across student, community, OCD, and clinical control samples (Cronbach’s α = 0.96, 0.90, 0.94, and 0.98, respectively) (Aardema et al., 2008). It has also shown good convergent and divergent validity, as well as strong test–retest reliability in student and clinical samples (Radomsky et al., 2006).
Statistical Analyses
In their study, Soffer-Dudek et al. (2015) found that several DES items loaded on multiple factors and that some were theoretically incompatible with the factors on which they loaded. They therefore developed a brief “purified” DA scale consisting of eight items consistent with the theoretical construct of absorption. This scale excludes items with factor loadings below .50 and those with less than a 10% difference in explained variance relative to other factors.
To test the first hypothesis, confirmatory factor analyses (CFA) were conducted by comparing a one-factor solution and the 18-item three-factor solution proposed by Soffer-Dudek et al. (2015). The 18 items were selected based on their CFA and structural equation modeling results and included the eight-item purified DA factor (items 14, 15, 17, 18, 20, 21, 23, 24), depersonalization/derealization (items 7, 9, 11, 12, 13, 27), and dissociative amnesia (items 3, 4, 8, 26). Using a one-factor model with these same 18 items allowed for a direct comparison with the three-factor solution without confounding effects related to item removal.
Model fit was evaluated using standard criteria: non-significant χ² (p > .05), χ²/df < 2, RMSEA < .07, CFI and TLI > .95, and SRMR < .08. No model modifications were applied. Given the high skewness of some items and the 11-point response format of the DES, robust maximum likelihood estimation (MLR) was used instead of maximum likelihood.
The second hypothesis—that DA would predict OCD symptoms—was examined using correlational, partial correlational, and linear regression analyses, with OCD symptoms as the dependent variable and DA scores as the independent variable, controlling for depression. Additional regressions examined the prediction of specific OCD symptom domains using VOCI scores.
Finally, the third hypothesis—that individuals with OCD would show higher DA levels than clinical and non-clinical controls—was tested using ANOVA, with post hoc comparisons conducted via Tukey’s HSD and the harmonic mean applied due to unequal group sizes.
RESULTS
Descriptive Statistics
Means and standard deviations for the DES, BDI and VOCI are reported in Table 1 for each group of participants. Cronbach alphas suggest that the three scales were internally consistent, with a value of .92 for the DES, .94 for the BDI and .97 for the VOCI (Beck et al., 1996; Carlson & Putnam, 1993; Thordarson et al., 2004).
Hypothesis 1: Underlying factor structure of the DES
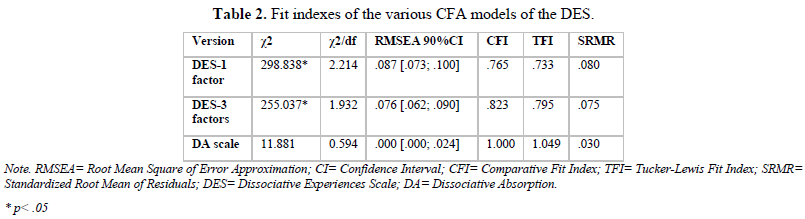
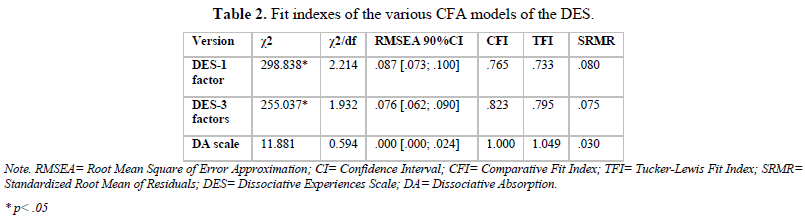
CFA in the OCD group showed that, while a slightly better fit than the one-factor solution, the three-factor solution of the DES (as found in Soffer-Dudek et al., 2015) was not an adequate fit of the data, as only two of the six fit indexes indicating good fit (see Table 2 for fit indexes). Inspection of the modification indices suggest that unrepresented cross-loading between items in the amnesia as well as the depersonalization/derealization factor resulted in poorer model fit. As well, loadings were low for items in the amnesia factor.
Given the poor fit of the three-factor solution, it was decided to test only the DA factor as this factor was found to be the most relevant to OCD symptoms (Soffer-Dudek et al., 2015). CFA results revealed that the model was an excellent fit for the data. All fit indexes indicated good or excellent fit: the chi-square test was significant, χ2/df was lower than 2, the RMSEA was lower than .07, CFI was higher than .95, TFI was higher than 0.95 and SRMR was lower than .05. The differences between Soffer-Dudek’s three-factor solution and the DA scale alone could be due in part by greater parsimony of the data (CFA penalizes more complex models) and subtraction of the DEP and AB scale.
Hypothesis 2: DA factor and the prediction of OCD symptoms
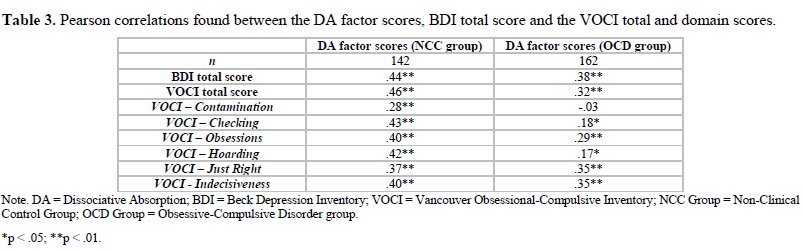
Table 3 presents the Pearson correlations found between the scores on the DA factor and the VOCI total scores and BDI scores. When limiting analyses to the NCC group alone, moderate correlations were found between these scores. When limiting analyses to the OCD group alone, correlations between the DA factor, the VOCI total scores and BDI scores remained significant but were numerically lower (r of .32 to .38) than the correlations found when using the NCC sample (r of .44 to .46).
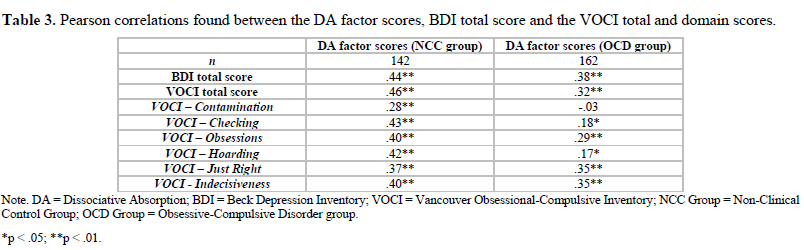
Pearson correlations found between the scores on the DA factor with specific OC dimensions are also presented in Table 3. When limiting analyses to the NCC group, moderately significant relationships were found between these scores, with the Checking domain as the strongest and the Contamination domain as the weakest. When limiting the analyses to the OCD group, moderately significant relationships were found between the DA factor and the Obsessions, Just Right and Indecisiveness domains, with weaker relationships found between the DA factor and the Checking and Hoarding domains. Moreover, correlation coefficients for the OCD group were numerically lower than the coefficients found between the DA factor and the OC domain scores for the NCC group.
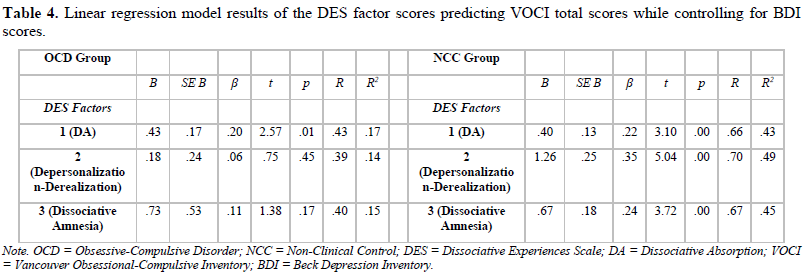
Table 4 presents result from the linear regressions that were performed to predict VOCI total scores based on the three DES factors taken individually while controlling for BDI scores. When limiting analyses to the NCC group, all models and predictor variables were significant (p < .05; R2 of .43, .49 and .45 for the DA, Depersonalization-Derealization and Dissociative Amnesia factors respectively). Conversely, when limiting analyses to the OCD group, only the model using the DA as the predictor variable was significant (p < .05; R2 of .17).
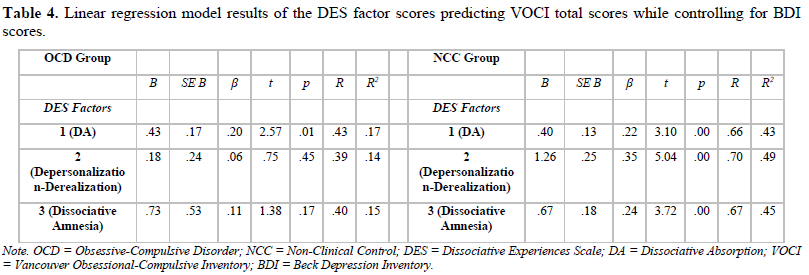
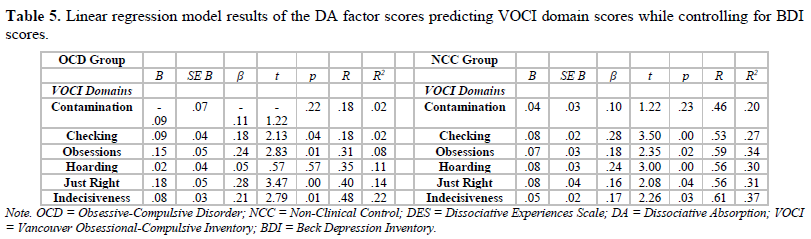
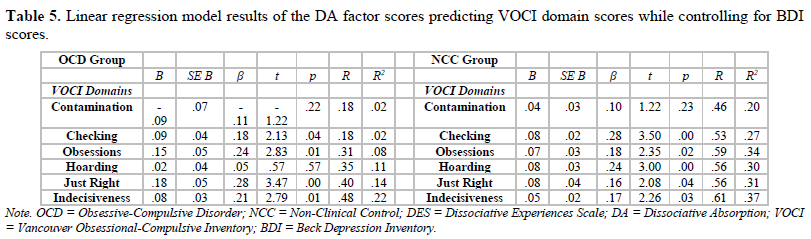
Table 5 presents results from the linear regressions that were performed to predict VOCI domain scores based on DA factor scores while controlling for BDI scores. When limiting analyses to the NCC group, the models for the VOCI Checking, Obsessions, Hoarding, Just Right, and Indecisiveness domains as predictor coefficients were statistically significant (p < .05). Conversely, when limiting analyses to the OCD group, only the models for the VOCI Checking, Obsessions, Just Right and Indecisiveness domains as predictor coefficients were statistically significant (p < .05). In addition, the variance explained by these four predictor coefficients was numerically lower in the OCD group (R2 of .02 to .22) than the variance explained by these same four predictor coefficients in the NCC group (R2 of .27 to .37).
Hypothesis 3: Differences between group mean scores on DA factor
A one-way between subjects ANOVA was conducted to compare the mean scores of the three participant groups on the DA factor. There was a significant difference found on the DA factor scores for the three groups (F(2, 325) = 4.84, p < .01). Post hoc comparisons using the Tukey HSD test indicated that the mean score for the mixed AD/DD group (M = 27.14, SD = 18.55) was significantly higher than the mean score for the NCC group (M = 16.53, SD = 14.30) and for the OCD group (M = 18.31, SD = 15.96).
DISCUSSION
The current study aimed to replicate the findings from Soffer-Dudek et al. (2015) by investigating the underlying structure of the DES in an OCD sample rather than a non-clinical sample. First, it was hypothesized that DA is a unique dissociative factor within a three-factor structure of the DES. Second, because DA was the only dissociative scale that longitudinally predicted OCD symptoms in non-clinical participants, it was hypothesized that the purified DA factor would significantly predict symptoms of OCD. Finally, it was hypothesized that those with OCD would score significantly higher on DA than clinical and non-clinical controls.
Unlike previous studies, this study investigated the underlying structure of the DES in an OCD clinical sample rather than only in a non-clinical sample to determine whether the three-factor model of the DES found by Soffer-Dudek et al. (2015) is supported and if the DA factor is a unique and clinically relevant dissociative tendency that is particularly significant in OCD symptomatology. While the three-factor model was not confirmed in this study’s OCD sample, the DA factor alone performed very strongly in the CFA. Thus, absorption is an empirically-derived unique dissociative factor that appears to be present in an OCD sample.
Our second hypothesis, namely that the purified DA factor would significantly predict symptoms of OCD, was confirmed in both the OCD and NCC groups. These results replicate the findings from Soffer-Dudek et al. (2015) where DA could predict OCD symptoms in non-clinical participants. An examination of the linear regression model revealed that the DA factor scores could significantly explain 17% of the total variance in OCD symptoms while controlling for depression in the OCD group, which represents a “large effect” (Cohen, 1988). The linear regression model revealed that the DA factor scores could significantly explain 27% of the total variance in VOCI Checking symptoms in the NCC sample. These findings are consistent with previous studies that report on dissociative symptoms significantly relating to checking symptoms (Grabe et al., 1999; Rufer et al., 2006; Watson et al., 2004). In addition, when limiting the analyses to the OCD group while controlling for depression, the DA factor scores were found to significantly predict VOCI Obsessions, Checking, Just Right and Indecisiveness symptoms and explained 2%, 8%, 14% and 22% of the total variance respectively. This gives further support to a theoretical hypothesis elaborated by Soffer-Dudek (2014) that absorption may be the dissociative factor uniquely associated with OCD symptoms.
However, our third hypothesis, namely that those with OCD would score significantly higher on the DA factor than clinical and non-clinical controls, was not supported. In contrast to expectations, the mixed AD/DD group was found to have a significantly higher DA factor mean score than both the NCC and OCD groups. Hence, although DA appears to be relevant to OCD symptomatology, those with OCD do not appear to show elevated levels of dissociative absorption. One explanation for these findings might be that DA primarily acts as an exacerbating factor in OCD symptoms, without elevated levels of DA being characteristic of those with OCD in general. While surprising given previous results, this is not inconsistent with the notion that DA is primarily the end-product of distorted inferential reasoning processes that lead the person to become highly absorbed into obsessions, and confuse reality with imagination (Aardema & Wu, 2011; Paradisis et al., 2015). A tendency to become easily absorbed at the exclusion of attention being paid to external stimuli may worsen OC symptoms to an important extent, or act as a vulnerability factor in the development of OCD, but at the same time, may not characterize those with OCD. Further experimental research is needed to establish causal connections between DA and associated cognitive processes like inferential confusion with OCD symptoms.

No Files Found




Internationally Accepted
Share Your Publication :