
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Nobuo Motegi*
Corresponding Author: Nobuo Motegi, Professor of Oral Health Science, Meikai University, 1 Akemi Urayasu Chiba, Japan
Received: December 30, 2021 ; Revised: January 17, 2022 ; Accepted: January 20, 2022 ; Available Online: April 30, 2022
Citation: Motegi N. (2022) Dental Health Wellbeing Including Hedonic as well as Eudemonic Wellbeing between Children and Adults. J Oral Health Dent Res, 2(1): 1-7.
Copyrights: ©2022 Motegi N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Abstract
Wellbeing comprising of hedonic and eudemonic wellbeing can be less likely to be seen in dentistry. Specifically, regarding dental health, dental symptoms including pain, discomfort, swelling, smell and appearance affects hedonic wellbeing. On the other hand, symptoms such as malnutrition, insomnia, growth and development affect eudemonic or eudaimonic wellbeing.
Objectives: To reveal how dental health affects children and adults’ wellbeing including hedonic and eudemonic wellbeing.
Methods: Two perspectives based on hedonic and eudemonic wellbeing in dental health are examined. In addition, with the examination of the number of citations from Public Medline or PubMed, they mainly are compared children with adult relevant to two wellbeing.
Results: It was significantly shown that the symptoms relevant to pain and appearance had a great influence on hedonic wellbeing in adults, while, the words relating to nutrition, growth, development, work, study and quality had a small impact on eudemonic wellbeing.
Conclusions: Dental health can benefit hedonic and eudemonic wellbeing. Specifically, hedonic wellbeing can enhance hope, joy and pride or pleasure fulfilment. On the other hand, eudemonic wellbeing can advance individual growth and positive thoughts in life or achievement of goal.
Key words: Dental, Health, Wellbeing, Hedonic, Eudemonic
INTRODUCTION
Good dental health is defined as not just the absence of disease but the sufficient ability to employ the mouth for daily life including communication tools such as smiling, speaking as well as eating functions such as tasting, swallowing, chewing and touching. Moreover, oral or dental health is essential not only for physical but also psychological health [1,2].
Dental health has a significant influence on general health. When dental health is compromised and harmful bacteria appears, it can incur an increment of risk for diseases such as cardiovascular disease or stroke. Furthermore, dental disease has been connected with complications in pregnancy, delivery and respiratory, gastrointestinal, rheumatologic, as well as immunological problems.
In addition, since the mouth is a primary role of personal appearance, oral health has distinct psychological and social factors [1,2]. Specifically, people with visible symptoms of oral disease are negatively evaluated and socially condemned with consequences to their psychological health as well as other effects on both hedonic and eudemonic wellbeing [3].
The World Health Organization (WHO) appreciates that dental health is essential to general health and considerable for wellbeing because it allows individuals to eat, speak, and socialize [4]. Dental problems generally cause pain and infection resulting in disease which might lead to the absence from work, school and a lack of sleep or appetite [5].
Dental health is considered a substantial part of health and wellbeing all over the world. Moreover, dental health is regarded as an indicator of extensive health and social care problems including nutrition and life-style related diseases such as obesity or systemic diseases caused by oral infection including diabetes and heart disease.
Dental diseases have been comparatively disregarded by policy makers and politicians regarded it as a minor problem. On the other hand, at a United Nations conference on prevention of non-infectious diseases, oral fields were focused on as a major universal public health precedence [6].
METHODS
Research methods are a quantitative approach. Two perspectives based on hedonic and eudemonic study are carried out. In addition, dental health is divided into two parts, children and adults, as a result, they can compare with two categories.
The search engine program is available to Public Medline or PubMed. The data from PubMed was gathered to investigate the number of citations. Specifically, relating to information retrieval, the different key words which contained information with relationship between hedonic or eudemonic words including pain, discomfort, swelling, insomnia and appearance relevant to hedonic wellbeing and nutrition, growth, development, work study and quality relevant to eudemonic wellbeing, 12 items and the category comprising children, young, adults, old or 4 items. Totally, 12 items multiple 4 items =48 items. After finding the results of the number of each category, the results were summarized.
RESULTS
The table was illustrated in descending order of the number of adults in Hedonic Wellbeing, the biggest number is 81 citations of pain, subsequently is 38 those of appearance, 23 those of discomfort, 3 those of swelling and each one these smell and insomnia respectively. Next, as for the number of citations for children in Hedonic Wellbeing, the biggest number is 29 citations of pain, subsequently is 30 those of appearance, 5 those of discomfort, 2 of insomnia respectively.
In relation to Hedonic Wellbeing, as the result of comparison ‘young’ with ‘adults’, the number of ‘young’ is bigger than that of ‘old’. On the other hand, the number of ‘children’ is smaller than ‘adults’ (Table 1, Hedonic Wellbeing).
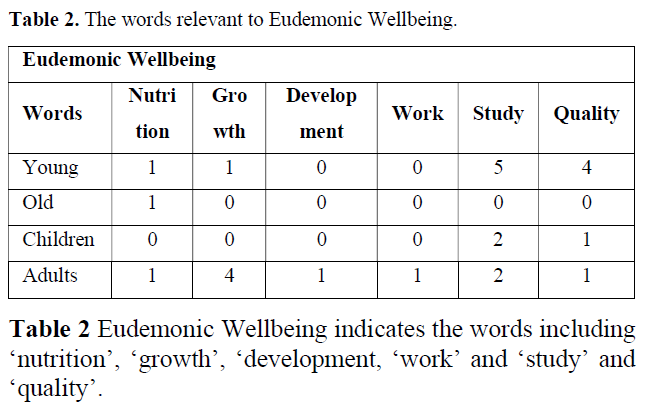
Compared to the number of citations relating to Eudemonic Wellbeing, those of Hedonic Wellbeing is significantly greater of numbers. However, the small number of those can be seen in Eudemonic Wellbeing. Specifically, it is listed that 5 citations of ‘study' and 4 those of ‘quality’ (Tables 1 & 2), Hedonic and Eudemonic Wellbeing). Additionally, 4 citations of 7 growth’, 2 those of ‘study’ one citation of ‘nutrition’,’ development’, ‘work’, ‘quality’ respectively. In addition, one citation of ‘nutrition in ‘old’ was listed (Table 2, Eudemonic Wellbeing).
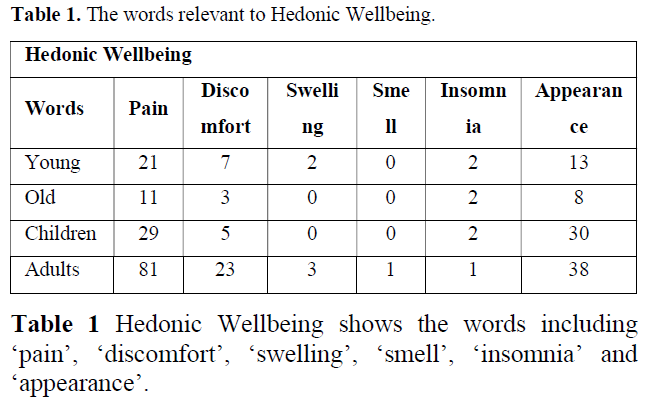
Regarding Hedonic Wellbeing, the most number of citations at 81 is ‘pain’ in adults. The least number of citations is 1 with ‘sell’ or ‘insomnia’ in adults.
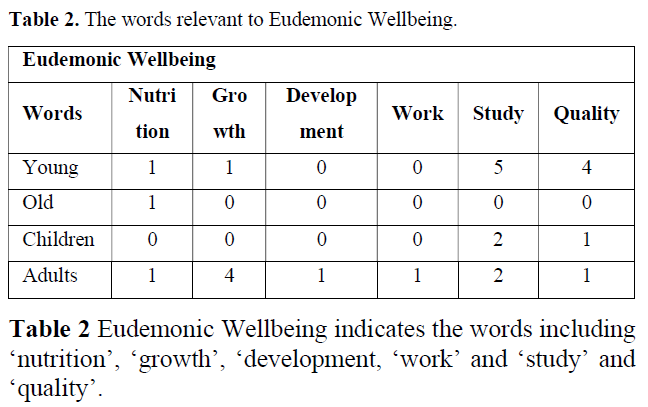
Concerning Eudemonic Wellbeing, the citations of the highest rate is 5 with ‘study’ in young, and that of the lowest rate is 1 with ’nutrition’ or ‘growth’ in young.
DISCUSSION
In terms of the citations of ‘Hedonic Wellbeing’, firstly ‘pain’, secondly ‘comfort’ and thirdly ‘discomfort’ can be seen. The feeling of pain as hedonic wellbeing is most likely to be considerably significant and gravely serious issues for people. Specifically, the majority of people would desire avoiding tooth or gingival pain because of severe pain.
Additionally, appearance is more likely to have a deep relationship with individuals as well as social lives. Specifically, almost all adults and also children are more likely to care about and mind their appearance and also as people take a caution about facial expression, they feel happy, sad and angry by other faces’ conditions. In addition, people are always concerned or care about how they appear to others.
Eudemonic wellbeing is a significant factor for people to simply to live or spend a quality of life.
With regards to Eudemonic Wellbeing, the number of citations of ‘study’ those of ‘growth’ and ‘nutrition’ can be seen. This is because that study is most likely to be indispensable for not only children but also adults. Specifically, if they suffer from tooth or gingival pain, they are less likely to be able to study hard.
Moreover, it is essential for children to grow up their body as well as mind. This is because that physical and mental growth is most likely to be vital for children or younger. Furthermore, good nutrition leads to enhance children’s growth. From now on, hedonic and eudemonic wellbeing relevant to dental health would be defined as follows: Wellbeing comprising hedonic and eudemonic approach in dental health, Dental health in children and wellbeing and Dental health in adults and wellbeing.
Wellbeing comprising hedonic and eudemonic approach in dental health
Recent research on wellbeing has come from two general points of views. One theory is the hedonic approach, which highlights happiness and gives a definition of wellbeing with regard to pleasure fulfillment and pain avoidance.
Another theory is eudemonia, which focuses on meaning and self-awareness and defines wellbeing relating to the degree to which a person is completely functioning, rational activity in accordance with moderation [7]. In other words, wellbeing is not just the absence of pain or displeasure but also when people have a meaning to accomplish substantial goals.
Aristotle (384-322 B.C.) introduced the concept of eudaimonia or eudemonia. In terms of Aristotle, eudemonia is an activity (energeia), not a state of mind, and an activity in agreement with virtue (kat’areten), worked over a lifetime in the existence of a sufficient number of external goods. Therefore, eudemonia is something substantially different from ordinary happiness, realized mainly as a state of spiritual satisfaction that is free from moral values. Eudaimonia (“happiness, “flourishing”), and turn to an examination on the nature of arete (“virtue”, “excellence”) and the character traits that human beings need in order to live life at its best [8]. Although the current hedonic idea exists, a majority of philosophers, religious authorities, visionaries all over the world have substantially disclaimed happiness as a fundamental norm of wellbeing relevant to eudemonia. Aristotle regarded hedonic happiness as a vulgar idea. He pointed out that true happiness can be expressed as virtue and namely, is to do what is worth doing [7]. Wellbeing is referred to in a wide variety of backgrounds and with various meanings comprising physical, social and psychological dimensions. Wellbeing is a positive physical, social and mental condition.
Additionally, people can take part in society, build up supportive personal relationships, strong and inclusive communities, good health, financial and personal security as well as a healthy and attractive life. Psychological wellbeing is a significant component of both mental and physical health [9].
Research has found that mental wellbeing can have a distinctive influence on enhancing physical health and promoting life expectancy.
Social networks as well as social capital, which will be discussed later on in the paper in detail, are essential elements for health and wellbeing. Wellbeing is significantly effective for public health including dental health. Wellbeing incorporates psychological health (mind) and physical health (body) in relation to more holistic approaches to disease and prevention of these as well as general health. Additionally, wellbeing brings about an outcome that is meaningful to the public [9].
Advanced psychology, neuroscience, and measurement theory implies that wellbeing can be led to accurate outcomes from cross-sectional, longitudinal and experimental studies. Specifically, wellbeing has a positive influence with longevity, psychological and physical health and social environment [10].
Wellbeing is substantially connected with a great deal of health. In detail, it deals with decreased risk of disease, injury, better immune system and increased longevity. Individuals with advanced levels of wellbeing are more productive at work and are more likely to take a part in their communities [11].
Concerning hedonic wellbeing, transient tooth pain and gingival swelling cause discomfort and irritation. Ameliorating pain and swelling bring about a comfortable and an appropriate mastication. Therefore, Alleviation of these symptoms can promote hedonic wellbeing or pleasure fulfilment.
On the other hand, regarding eudemonic wellbeing or achieving a goal and a moral life, severe or serious pain and swelling could cause insomnia resulting in or a lack of sleep, malnourishment and an absence of school and work. Moreover, periodontal diseases are more likely to cause systemic diseases including diabetes and heart disease. These situations incur in the deterioration of eudemonic wellbeing. In consequence, holistic approach is needed.
Dental health in children and wellbeing
Good oral or dental health in childhood is an essential element in enhancing the life time of oral as well as general health. Dental disease in young children can have a significant serious influence on their health and wellbeing [12]. It might comprise insufficient sleeping, unstable eating and afflicted daily activity such as refusing food and interrupted learning at school [13].
An increment of concern could be seen in the possible connection between tooth decay and obesity. Younger children had a tendency in the reduction of growth and weight when they had serious tooth decay in early stages in their life [14]. Younger children could not eat food appropriately and as a result, they became malnourished and also had a lack of sleep and in some cases, they had insomnia. Severe tooth decay influences growth and wellbeing [14]. Two greatly related systematic reviews can be seen in children included the connection between tooth decay and body weight condition. In one review, Hayden [15] found that children who were overweight had a higher rate of tooth decay compared to no-overweight children. Another review, which Hooley [16] conducted, found that obese children had a higher rate than no obese children in terms of tooth decay.
Banihani [17] revealed that the influence of tooth decay and its treatment on oral health had a deep relationship with the quality of life and wellbeing of children and families. The authors surveyed the effect of the oral health in relation to quality of life of the children with untreated tooth decay aged between 4 and 9 in the UK. In consequence, tooth decay had a correlation with negative effects on children and parents’ quality of life. On the other hand, tooth decay treatment substantially promoted the quality of life of children and families and wellbeing.
Specifically, children’s subjects’ questionnaire revealed school absences, inability to concentrate in school, reduced self-esteem, insufficient social correlation, affected speech development, a lack of sleep and malnutrition. A report by parents included toothache, mouth and jaw pains, irritations or frustrations, difficulty eating and insomnia.
Dental problems have a substantial impact on not only the growth but also cognitive development of the child in the long periods due to malnutrition. This condition can lead to lower weight and height in terms of the growth of the body. Additionally, serious tooth decay has a substantial effect on families. As a result, sleepless nights, lost workdays for caregivers or time and financial influence on the families.
Regarding hedonic wellbeing, when children can eat delicious food and be satisfied with this condition. Consequently, they can feel excitement and enjoyment and have a comfortable time or pleasure fulfilment temporarily. Concerning eudemonic wellbeing, after the treatment of tooth decay, children can improve their mastication capacity, as a result, they can absorb nutritious food and this can lead to the recovery of malnutrition. Consequently, they can produce normal growth physically as well as cognitive development psychologically. Additionally, they can attend their school and communicate with each other and they can study their subjects and can accomplish their goal or a good achievement and moral life.
In general, a majority of children suffered from tooth decay in early childhood. What is more, children with cleft lip and plate have an extensive as well as serious tooth decay. Children who suffer from cleft lip and palate have various problems in relation to eating, communication and appearance psychologically and socially. Specifically, these problems frequently extend to adolescence with appearance and speech problems According to Smallridge [18] to investigate fluoride treatment and oral health conditions and to survey the connection with the region risk factors with tooth decay in cleft care in the UK. As a result, 75 children (29%) had rampant caries or severe or extensive tooth decay and 138 children (54%) had at least one incisor with dental anomalies and 10% had at least one tooth extracted.
Prescriptions were 10% with fluoride tablet and 23% with fluoride vanish, respectively. Exclusively 29 children (11%) with a high fluoride concentration, the majority (84%) of children were with low levels of fluoride. Children had high levels of tooth decay, rampant tooth decay and incisor anomaly. In consequence, a high proportion of tooth decay, serious or widespread tooth decay and enamel incisor anomalies could be seen.
Cleft palate patients might need to be immediately treated due to rampant caries or severe tooth decay and also children who have a facial or mouth region deformity including cleft lip and palate can exacerbate psychological and physical health and wellbeing. With regard to hedonic wellbeing, cleft lip and palate children cannot eat sufficient food seriously and become severely malnourished. Adolescent young women with facial deformity have higher proportions of social adaptation problems, especially, appearance. If they can have better teeth, and could eat favorite food sufficiently and can feel comfortable to be able to experience food taste under five taste sensations including sweet, sour, bitter, salty and umami due to good mastication and also, they can be satisfied with aesthetics around mouth and a part of their face in public. In other words, improvement not only mastication but also aesthetics can advance social integration due to the recovery of communication and restoration of self-confidence.
These can lead to hedonic wellbeing or a pleasurable life and eudemonic wellbeing or a goal accomplishment.
It is difficult for a dentist to treat promptly and appropriately extensive and progressive tooth decay as well as gingival inflammation. Younger children frequently have a large amount of tooth decay due to excessive sugar intake. Moreover, dental phobia patients occasionally suffer from tooth decay due to avoidance of regular visit of dentist. These patients might have numerous and serious tooth decay which is likely to be irreversible as they have not been to the dentist to be treated. Children and their families might need treatment of severe tooth decay under general anesthesia in a hospital. The most common reason for the need for various extractions in younger children are dental phobia and learning disabilities. In England, approximately 43,700 children in 2015-16 aged 16 and under visited the hospital for the extraction of a tooth or for dental treatment of multiple teeth under general anesthesia.
Knapp [19] surveyed that tooth decay is substantial influence on children and parents and may need to be treated under general anesthesia. Research in children under 16 years old having treatment for tooth decay under general anesthesia was considered. For the oral health-related quality of life (a systematic review), two questionnaires were used. One was the early childhood oral health impact scale [20], another one is the parental caregivers’ perceptions of child oral health related quality-of-life questionnaire [21]. Two samples of the questionnaire’s answers are illustrated as follows:
Low [20] reported change in presence of manifestations as follows: presence of pain reduced from 48% to 3%, problems eating reduced from 43% to 3%, 84% improved sleeping.
Thomas & Primosh [21] reported complaints about teeth from 56% to 2%, chewing problems 60% to 8%, eating less 52% to 4%, sleeping problems 30% to 4%. Treatment under general anesthesia seems to lead to overall improvements in oral health-related quality of life and wellbeing.
Usage of general anesthesia can acceleratingly ameliorate tooth pain. Prompt alleviation for pain can enhance quality of life and wellbeing.
When children can eat a great amount of food, they can feel full or pleasure fulfillment after a meal.
Promoting chewing and eating food can bring about the normal physical and mental growth or a good achievement and moral life.
Dental health has a great influence on eudemonic as well as hedonic wellbeing and it can affect how children grow, look, speak, chew, taste food and socialize physically and psychologically. Good dental health wellbeing can encourage children to begin the best condition in their early stage.
Dental health in adults and wellbeing
Systemic diseases can have direct and indirect influences on oral health; similarly insufficient oral or dental health can affect general health and wellbeing. A lack of oral care leads to the increment of dental plaque and calculus, which ultimately incur the development of tooth decay and periodontal disease, halitosis or bad breath, Toot loss and finally reduced oral function.
The physical health with serious psychological problems has been the highlight of growing attention, especially relating to diabetes, cardiovascular disease and chronic lung disease. A shortage of attention in terms of oral health problems bring about the chronic diseases. In addition, insufficient oral health can influence eating, speech and other social and psychological life and wellbeing.
PD arises exclusively in the existence of dental plaque and it begins with gingivitis (gum inflammation). The gums become separated from the teeth due to the symptom comprising bleeding gums and deeper pockets.
Gum inflammation scattered to the tissues and destroys the connective tissues and the bone. As a result, the disease is irreversible and it is frequently connected with halitosis.
In particular, poor oral hygiene arises halitosis because of bacteria inhabitants in gums and tongue. Cleaning the tongue and cleaning the teeth can help mitigate bad halitosis. Other causes of halitosis include food, drink, smoking, crash dieting and some medicines. In detail, strong smelling food such as garlic, onions and spices and drinks such as coffee and alcohol can also cause halitosis. Crash dieting such as fasting and low-carbohydrate diets incur halitosis because food brings about chemicals called ketones that can be smelled on the breath.
Halitosis is caused by other medical diseases such as diabetes, lung, throat and nose infections. Some patients under the misunderstanding are convinced they have bad breath when they do not have this condition. This psychological problem is called halitophobia. They are paranoid with regard to the smell of their breath. Treatment for halitophobia involves talking therapies such as cognitive behavioral therapy. Bad breath can deteriorate life satisfaction and individual and social life and wellbeing. Specifically, patients who suffer from frequent, foul oral smells can suffer from an inferiority complex and these smells occasionally lead to irritation not only from friends but also co-workers.
Moreover, the view of social function might be influenced due to comparatively general oral problems such as tooth loss. In this research of the older adults with tooth loss in the UK, 30% reported chewing problems [10].
Though only 5% improved their diet, 9% appeared uncomfortable chewing in front of others and 13% reported difficulty during social interaction. According to Fisk cited by NIH [10], 25% of people without teeth reported that they had averted close relationships with friends and co-workers due to fear of refusal when friends and co-workers realized they were toothless. The authors indicated that the responses to tooth loss by older adults comprised lowered self-confidence and renewed self-image, reluctance of appearance and the recognition of being more senior in age.
Relating to older adults who have tooth loss or are toothless, they have to wear dentures to eat food and they cannot usually their favorite food, especially tough and chewy ingredients. In addition, when some patients wear dentures, they change their appearances and several denture users might have deteriorated facial expressions. In accident, someone is more likely to be liable to swallow a small denture. An appropriate or tailored denture can lead to not only hedonic but also eudemonic wellbeing because those people can have no pain and good oral condition as well as good social integration.
The research investigating 3000 homes in Great Britain in terms of the influence of oral health on the quality of life was conducted. 70% of participants revealed that their oral health influenced their quality of life, not only positively but also negatively. The adults in higher socioeconomic groups, in particular, those who had seen a dentist within the last year, were more likely to show a promoting influence of oral health on the quality of life.
For tooth loss in relation to oral deformity, some cleft lip and palate patients have been given a prosthesis as the final restoration. They have not suffered from bone grafting because of the extensive defect and prosthodontic treatment or denture procedure. The improvement of TL can enhance oral health and quality of life as well as wellbeing. He remodeling due to denture can bring about a long-term mastication. Therefore, patients can absorb nutritious food for a long time. In addition, they can improve their appearance in their life. They can be willing to communicate with friends and co-workers and incorporated with social groups. As a result, they can accomplish their goals and aims in life. These can lead to eudemonic wellbeing or a good achievement and morale life.
According to Rouxel, dental disease including tooth loss have a substantial negative influence on the quality of life and well-being of older adults. Their research analyzed the connection between oral-related quality of life and loneliness amongst older adults living in England. The data showed participants aged 50 and older analyzed from 2006 to 2011.
The authors hypothesized that insufficient oral health will be integrated with considerable levels of loneliness and will have a negative effect on social involvement, social support and depressive manifestations. The results of this research have unveiled that a robust correlation between oral problems and loneliness in elderly English adults.
Loneliness can influence people at every age of life. However, the elderly in particular, those more than 80 years of age are at a higher risk of suffering from loneliness. International research has assessed that between 20% and 30% of people from 45- to 79-year-old how moderate or high loneliness in England. On the other hand, the portion of loneliness among those more than 80-year-old can illustrate from 40% to 50%. Exacerbating health might influence an individuals’ competence to sustain their daily lifestyle duties comprising social integration. Dental problems including tooth loss have a substantial negative effect on quality of life and wellbeing of older adults including functional, psychological and social importance. Good oral health is significant for social intercorrelation and general wellbeing.
Enhancement of mastication and appearance can lead to eudemonic as well as hedonic wellbeing comprising positive wellbeing in an increment of happiness, pleasure, purpose in life, life satisfaction and quality of life to prevent physical and psychological problems.
Specifically, older adults are frequently vulnerable and might request help to keep their independence and to gain confidence in oral health functioning comprising everyday life activities such as eating, communicating and smiling.
CONCLUSION
Good dental health can lead in a great direction, hedonic and eudemonic wellbeing. Specifically, hedonic wellbeing including the ameliorating of tooth pain, discomfort and appearance can enhance hope, joy and pride or pleasure fulfilment. On the other hand, eudemonic wellbeing comprising study, growth, development, work and quality can advance individual growth and positive thoughts for children and adults in their lives or achievement of their goals.
ACKNOWLEDGEMENT
I am grateful to Professor Charles Watters and Dr Tish Marrable, Social Work and Social Care University of Sussex for helpful discussions and comments on the manuscript.


REFERENCES
No Files Found




Internationally Accepted
Share Your Publication :