
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Marwan Abou-Rass*, DDS, MDS, Ph.D.
Corresponding Author: Marwan Abou-Rass, USC. Prof Emeritus, Founder of AbouRass Endodontics Academy (www.abourass.com)
Received: June 17, 2026 ; Revised: June 20, 2026 ; Accepted: June 22, 2026 ; Available Online: June 23, 2026
Citation: Abou-Rass M. (2026) The 4R Operational Diagnosis Protocol: R2 – The 10 ADIs Radiographic Interpretation System (10 ADIs-RIS). J Oral Health Dent Res, 5(3): 1-10.
Copyrights: ©2026 Abou-Rass M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Introduction: AbouRass’s 4R Operational Diagnosis Protocol (4ROD) integrates systematic physical assessment with the "10 Areas of Diagnostic Interest" (10 ADI-RIS) radiographic interpretation system. This structured approach evaluates anatomical landmarks—from the clinical crown to adjacent structures—to identify endodontic and periodontal pathology. Recognizing that radiographs are diagnostic aids rather than standalone definitive tools, the 10 ADI-RIS minimizes clinical error by grounding imaging in biological reality. It promotes disciplined, consistent interpretation, ensuring treatment planning is evidence-based, preventive, and clinically responsible.
Methods: The 10 ADI-RIS utilizes a systematic, sequential analysis of periapical and bitewing radiographs, focusing on ten specific anatomical landmarks (clinical crown, pulp chamber, root canal, apex, lamina dura, periodontal ligament, periapical bone, periradicular bone, alveolar crest, and adjacent anatomy). This protocol integrates radiographic findings with clinical data from the 4R Operational Diagnosis steps (R1, R3, and R4) to correlate images with biological reality, ensuring diagnostic accuracy and preventing reliance on subjective or isolated imaging.
Conclusion: The 10 ADI-RIS transforms radiographic interpretation from a subjective observation into a disciplined, error-reducing diagnostic science. By acknowledging the biological and technical limitations of two-dimensional imaging, this structured protocol ensures that clinicians look beyond isolated sites to assess the tooth and periodontium holistically. When integrated into the 4R Operational Diagnosis Protocol, the system significantly improves diagnostic reliability, facilitates interdisciplinary treatment planning, and promotes patient-centered, biologically justified decision-making in clinical endodontics and periodontics.
Keywords: 4R Operational Diagnosis Protocol, 10 ADI-RIS, Radiographic Interpretation, Endodontics, Periodontics, Diagnostic Accuracy, Clinical Decision-Making, Biological Reality.
#J Oral Health Dent Res has interviewed Dr. Marwan Abou-Rass regarding 4R Operational Diagnosis Protocol.
INTRODUCTION
The 4R Operational Diagnosis Protocol 4ROD is a clinical diagnostic approach developed by AbouRass (1982)*. It emphasizes a systematic, physical assessment of the tooth, pulp, and supporting tissues. The protocol consists of four steps:
R1: Patient’s Report and Rapport Findings
R2: Radiographic Findings
R3: Pulpal and Periodontal Response Testing
R4: Restorative and Tooth Structure Findings
Findings from these four steps are integrated to develop a problem list, establish a definitive diagnosis, and guide treatment planning.
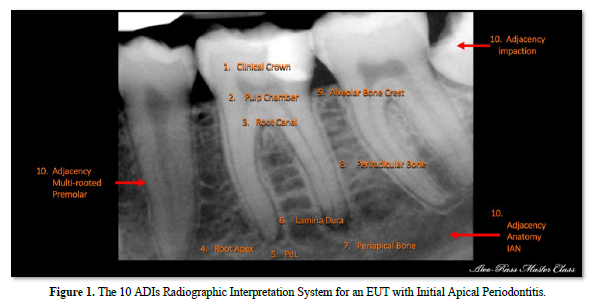
This article highlights the R2 step: the 10 ADI Radiographic Interpretation System (10 ADI-RIS). This system uses tooth-anatomy landmarks to assess factors that directly or indirectly influence the clinical and biological health of the tooth and its supporting tissues. It applies to both untreated endodontic teeth (EUT) and endodontically treated teeth (ETT).
The system guides clinicians through 10 sequential Areas of Diagnostic Interest to identify disease, treatment deficiencies, procedural errors, restorative concerns, periodontal complications, and hidden issues involving adjacent teeth or critical anatomical structures.
Q1. Why is Radiographic Interpretation a Critical Component of the 4ROD Protocol?
Clinical visual and tactile examination offers a limited value in the assessment of endodontic and periodontic problems. We all know that radiographic assessment is the standard of care; however, the question is: what is the best way to identify and quantify these problems?
Periodontal surgical research has demonstrated that surgical exploration not only identifies the problem but also allows precise measurement, making surgical measurements the gold standard.
Research has also shown that periapical radiology measurements closely approximate surgical measurements, though they are known to underestimate the presence, extent, size, and severity of dentoalveolar disease. Consequently, I do not treat radiographs as a standalone diagnosis. They are diagnostic aids, not definitive diagnoses. For this reason, in the 4ROD Protocol.
Q2. What are the Ten Areas of Diagnostic Interest – 10 ADIs
An area of diagnostic interest is an anatomical landmark or zone that directly or indirectly influences the biological or clinical treatment of the tooth and its supporting structures.
To identify these areas effectively in clinical practice, I rely on periapical radiographs as the most efficient and accurate imaging method for this system, supplementing with CBCT when needed.
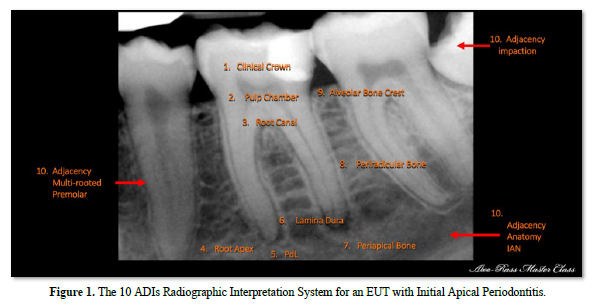
The 10 key areas include the clinical crown, pulp chamber, main root canal, root apex, lamina dura, periodontal ligament space, periapical bone, periradicular bone, alveolar bone crest, and neighboring teeth or critical anatomy.
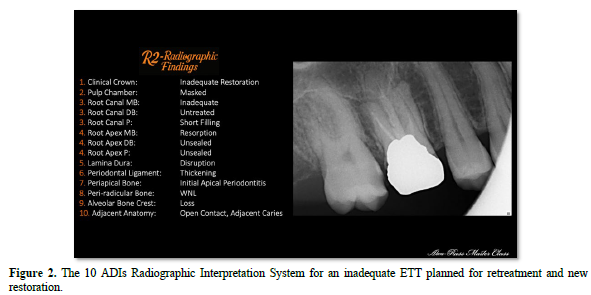
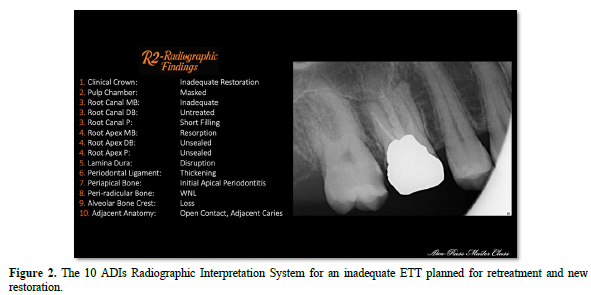
This method applies to both Endodontically Untreated Teeth (EUT) (Figure 1) and Endodontically Treated Teeth (ETT) (Figure 2). The 10 ADI system promotes a disciplined diagnostic approach.
By following a consistent pathway, I reduce the risk of missing important findings. For me, the 10 ADI-RIS is a structured, systematic, preventive, and error-reducing system for radiographic interpretation.
Q3. What is the Significance of Radiographic Findings within the 4ROD Protocol?
The 10 ADI-RIS is founded on a key principle: Radiographic findings are valuable but not sufficient on their own. While a radiograph can reveal structural changes, it cannot fully assess the biological condition of the tooth's endodontium or the health of its periodontium.
Diagnostic errors often happen when clinicians rely too heavily on images beyond their biological or technical limitations. Importantly, the absence of radiographic evidence does not mean the disease is not present.
I base the 10 ADI system on five core principles:
These principles direct my application of the 10 ADI system within the 4R operational diagnosis protocol. The goal is to correlate radiographic images with the patient’s biological reality and disease processes, ensuring interpretation is meaningful, grounded in biology, and minimizes errors.
Q4. Why do you rely on Periapical Radiographs when CBCT is Typically Considered the more Advanced Imaging Standard?
I rely on periapical and bitewing radiographs because they remain essential tools in routine dental diagnosis, particularly in endodontics, periodontics, and prosthodontics. When obtained with proper technique and high image quality, they offer valuable information that aids in diagnosis and treatment planning.
The advantages of periapical radiographs include:
I do not view periapical radiographs and CBCT as competitors but as complementary tools. CBCT is advantageous when conventional radiographs are inadequate or when three-dimensional information is clinically necessary. The key is to use CBCT selectively, not routinely, since more imaging does not automatically improve diagnosis.
The main caution is that clinicians must understand both the technical and biological limitations. While technical issues can usually be corrected, neglecting biological constraints can lead to misdiagnosis, unnecessary treatments, and professional negligence. Therefore, I rely on periapical radiographs within a structured diagnostic protocol rather than as standalone images.
Q5. What are the Biological and Technical Limitations of Periapical Radiographs?
Technically, conventional intraoral radiography compresses three-dimensional anatomy into a two-dimensional image, so anatomical structures and disease patterns may be superimposed, distorted, obscured, or missed entirely.
Biologically, radiographs show mineralized tissue changes only after the disease has produced enough structural alteration or damage to become visible. This means that a normal-looking image does not always represent biological health. Classic histologic-radiographic correlation studies highlight several key limitations:
For that reason, I do not interpret intraoral radiographs in isolation. In the 4ROD model, the 10 ADIs system provides a structured way to consistently review the image, accounting for R1, R3, and R4 findings.
Q6. Do all 10 ADIs Carry Equal Weight when Reviewing a Radiograph?
The significance of each ADI depends on how much it deviates from what I define as Within Normal Limits (WNL). Therefore, understanding what is considered normal is essential for accurate interpretation. This information is detailed in the PowerPoint presentation for each ADI in the Academy curriculum. For example, the importance of certain ADIs varies:
Q7. Please Explain How to Use Each of the 10 ADIs.
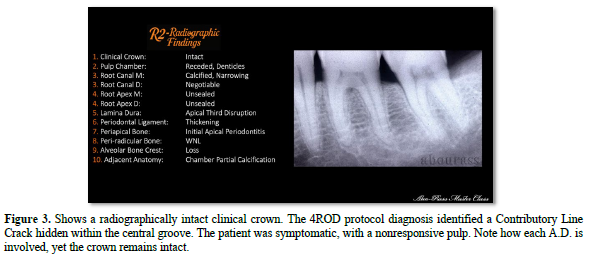
ADI 1: Clinical Crown
Clinical Crown assessment is categorized into three groups: radiographically unrestored crowns, radiographically restored crowns, and crowned teeth. In these three categories, the assessment of the interproximal contact his biologically and clinically most important.
In crowned teeth, the periapical radiograph is of limited usefulness because the crown obscures the prepared crown structure and the pulp chamber. To overcome this limitation, I use bitewing radiographs, which precisely show crown margins and their proximity to the alveolar bone crest. Additionally, I pay attention to what I term the 'halo effect,' which I clinically verify using a sharp explorer to detect recurrent caries, decalcification, or open margins.
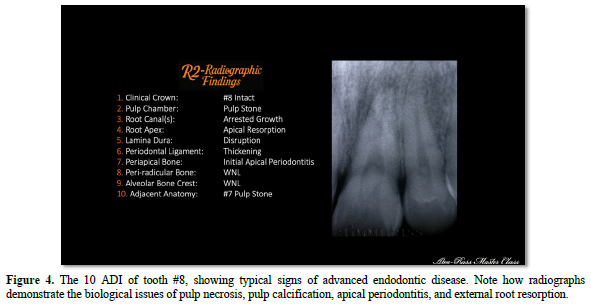
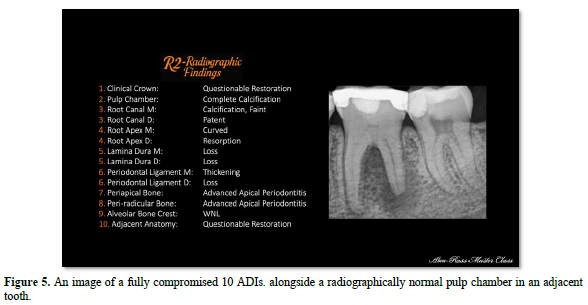
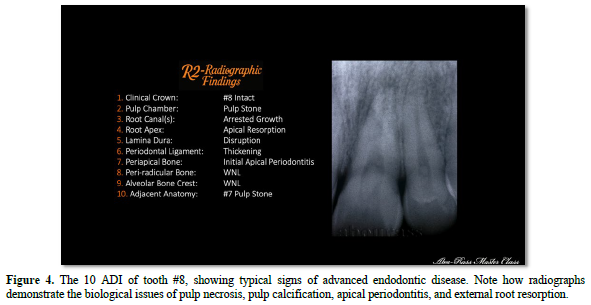
ADI 2: Pulp Chamber
Biologically, the pulp chamber acts as an indicator of pulp health. ADI 2 reviews the factors related to the pulp chamber before, during, and after endodontic treatment.
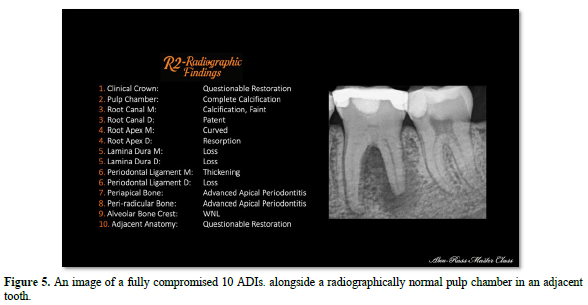
Radiographically, seven criteria are used to evaluate the pulp chamber:
These criteria are essential for diagnosis and endodontic procedures and apply to both untreated and treated teeth. They inform decisions regarding vital pulp therapy, crown preparation, and orthodontic movements. Figures 4 and 5 illustrate images of teeth in which the seven criteria have been affected.
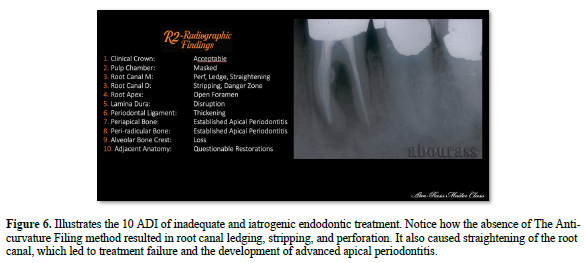
ADI 3: Root Canal
With ADI 3, I assess the main root canal space, recognizing that lateral canals, fins, and isthmuses are not visible either because of their microscopic nature or because of the two-dimensional nature of the radiograph.
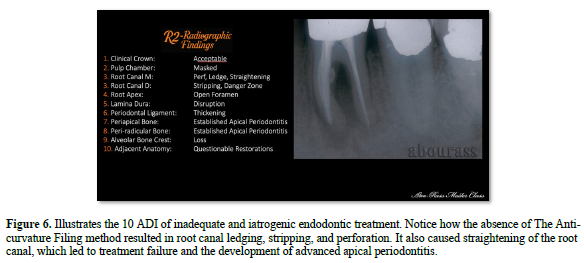
During the evaluation of the EUT, I assess the integrity of the root structure, its length and curvature, danger zones and safety zones, the radiolucency or opacity of the root canal, and signs of resorption.
When assessing ETT, I analyze the relationship between the root canal and the pulp chamber, including the chamber seal or posts, filling, canal flow, filling density, the seal, width, material type, stripping, and perforation. (Figure 6) The primary advantage of ADI 3 is that it reminds me that radiographic canal anatomy is a guide, not an exact map. I verify my interpretation clinically through canal negotiation and exploration.
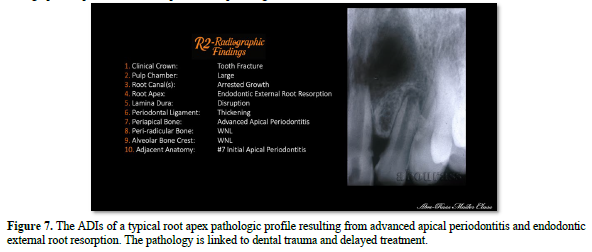
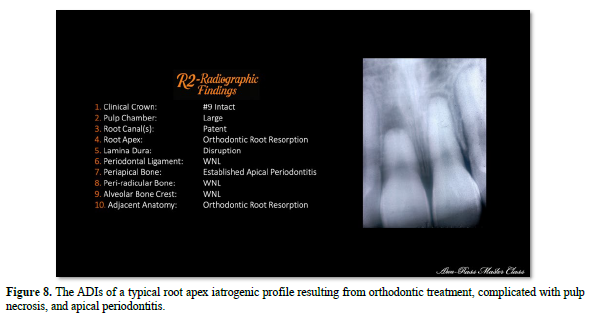
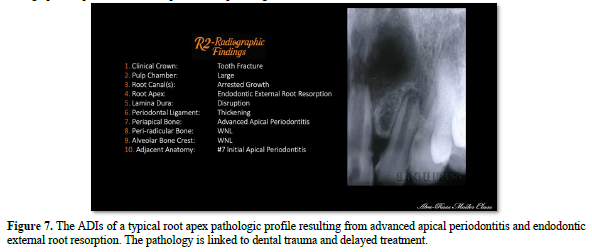
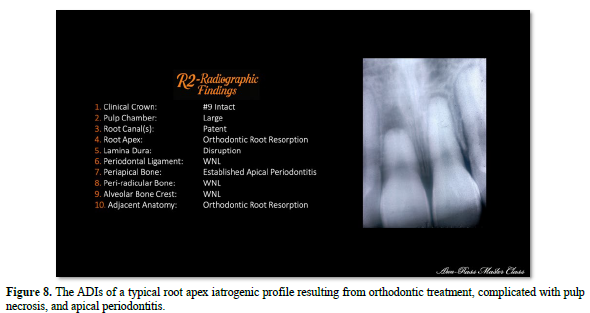
ADI 4: Root Apex
Regarding the earlier question about the weight of each ADI, the root apex exemplifies a critically important ADI. Biologically, the shape of the apex and the condition of the apical foramen influence both clinical and radiographic signs.
Anatomically, the shape affects root canal preparation procedures, determining the size and termination of the preparation.
Biologically, the root apex can display five different radiographic profiles: developmental, pathological, iatrogenic, adequate, and inadequate endodontic treatment. The PowerPoint presentation provides detailed clinical examples of these profiles. Of particular importance is the relationship between the filling and the apex.
A gap over 3 mm or material extruded beyond the apex may suggest endodontic treatment failure, especially when associated with symptoms, clinical signs, or periapical changes.
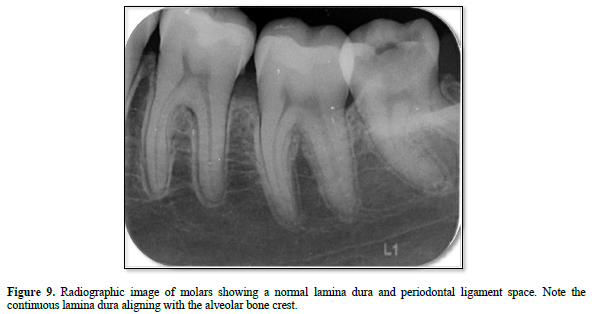
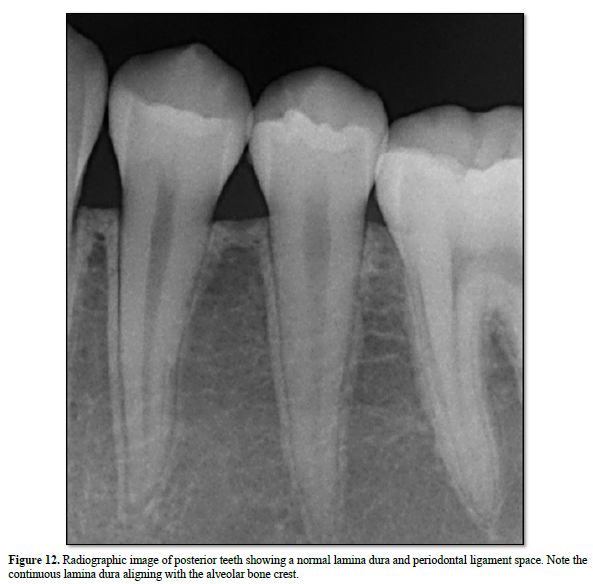
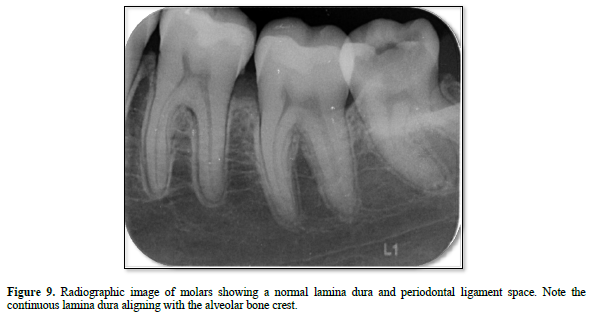
ADI 5 and ADI 6: Lamina Dura and Periodontal Ligament
With ADI 5 and ADI 6, I examine the lamina dura and periodontal ligament space, which are among the most sensitive radiographic indicators of pulpal, periodontal, occlusal, and periapical biologic and pathologic changes.
Loss of lamina dura continuity, widening of the periodontal ligament space, or loss of these features helps me identify disease and distinguish between endodontic and periodontal involvement.
Generally, intact lamina dura indicates health, while disruptions may signal pathology, trauma, occlusal stress, periodontal disease, or systemic factors.
I also view ADI 5, ADI 6, and ADI 9 as interconnected because the lamina dura extends upward into the alveolar crest Figure 9.
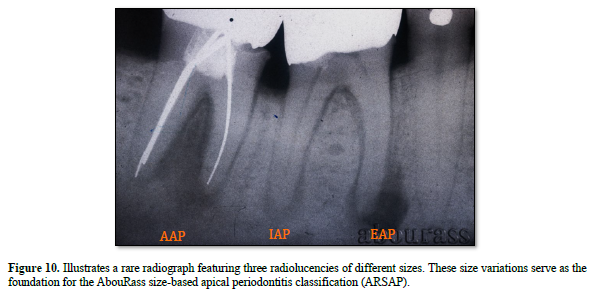
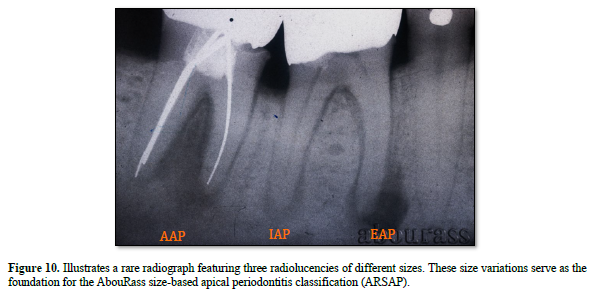
ADI 7: Periapical Bone
Using ADI 7, I assess the periapical bone surrounding the root apex for radiolucent changes associated with factors such as microbial toxins, inflammation, immune response, or host defense. On X-rays, these changes may appear as a loss of normal bone around the apex or alterations in trabecular bone structure, ranging from severe radiolucency to opacity. This ADI helps me categorize the size and scope of periapical disease:
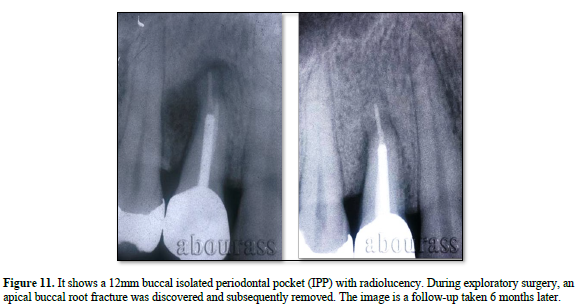
ADI 8: Periradicular Bone
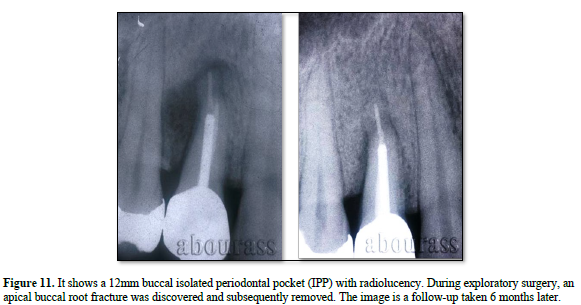
ADI-8 was added to the system to distinguish between endodontic and periodontic pathology. ADI 8 covers the periradicular, furcal, and interdental bones, which may present as periodontal problems. The pathology of concern is called an Isolated Periodontal Pocket (IPP)
Many lesions in the periradicular bone in both EUT and ETT are due to pulpal or endodontic issues, such as pulp necrosis, tooth structure cracks, untreated root canals, and root perforations. These are often mistaken for periodontal diseases.
A key difference between IPP and periodontal pathology is that the isolated periodontal pocket heals after addressing the endodontic cause.
ADI 9: Alveolar Bone Crest
The alveolar bone crest (ABC) is a part of the socket lamina dura, and its loss can negatively impact the tooth’s pulp and periodontal health.
The most common cause of ABC loss is interproximal restorative discrepancies, including inadequate restoration contours, overhangs, and open margins. Additionally, ABC loss is linked to systemic diseases.
The advantage of ADI 9 is that it relates radiographic findings to periodontal health status, serving as a marker of periodontal health. Bitewing radiographs typically provide the clearest view of the alveolar crest, making them especially useful for assessing crestal bone levels and interdental changes.
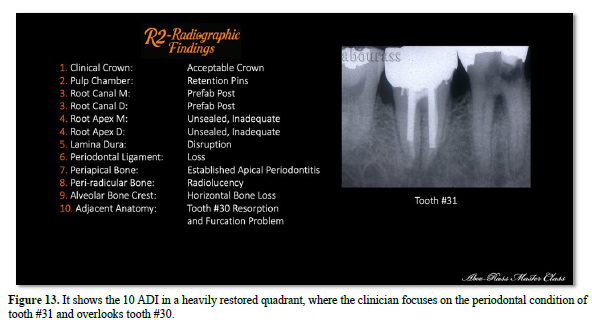
ADI 10: Adjacent Teeth and Anatomical Structures
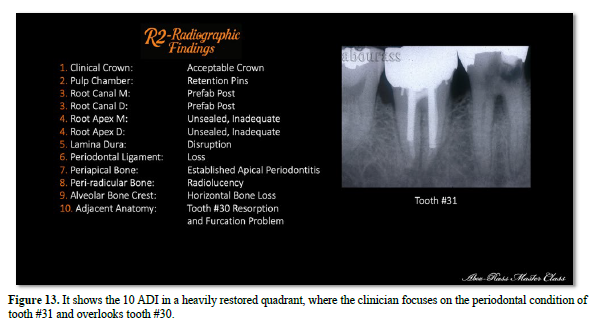
Heavily restored dental quadrants may harbor hidden chronic issues that could flare up during endodontic or restorative procedures on adjacent teeth. Concluding the 10 ADIs assessment with the evaluation of neighboring teeth helps prevent misdiagnosis, treatment complications, and patient dissatisfaction.
This assessment also considers vital nearby structures, including the maxillary sinus, the inferior alveolar neurovascular bundle, the nasal floor, and the incisive canal. The primary advantage of ADI 10 is its preventive nature. Focusing solely on one tooth risks missing other issues. By examining adjacent teeth and surrounding anatomy, I offer a more thorough, patient-centered, and clinically responsible interpretation, Figure 13.
CONCLUSION
The 10 ADI Radiographic Interpretation System (10 ADI-RIS) transforms radiographic interpretation from a subjective observational exercise into a structured, systematic, and biologically based diagnostic process. Rather than focusing on isolated radiographic findings, the clinician evaluates ten sequential anatomical areas that collectively influence the health and disease of the tooth and its supporting tissues.
The greatest strength of the system lies not only in its organization but in its integration within the 4R Operational Diagnosis Protocol. Radiographic findings (R2) are interpreted together with the patient's history and clinical findings (R1), pulpal and periodontal response testing (R3), and restorative and tooth structure assessment (R4). This comprehensive approach minimizes diagnostic errors, improves communication among clinicians, supports interdisciplinary treatment planning, and promotes biologically justified, patient-centered clinical decision-making.
The 10 ADI-RIS is not intended to replace clinical judgment; rather, it provides a disciplined framework that helps clinicians consistently identify significant radiographic findings while recognizing the biological and technical limitations of imaging. Radiographs are indispensable diagnostic aids, but they do not establish the diagnosis on their own.
Ultimately, radiographs demonstrate anatomy, whereas biology explains disease. The purpose of the 10 ADI-RIS is to bridge these two realities, ensuring that radiographic interpretation becomes clinically meaningful, biologically relevant, and an integral part of comprehensive diagnosis through the 4R Operational Diagnosis Protocol. Radiographs demonstrate anatomy; biology explains disease.


No Files Found




Internationally Accepted
Share Your Publication :