
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein DMD, MS*
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: May 13, 2026 ; Revised: May 15, 2026 ; Accepted: May 16, 2026 ; Available Online: May 17, 2026
Citation: Millstein PL. (2026) The Clinical Value of a Balanced Bite. J Oral Health Dent Res, 5(3): 1-4.
Copyrights: ©2026 Millstein PL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Electronic devices record contact pressure and force numerically. Do the extrapolated findings relate to the familiar blue paper contact marks? Is a balanced bite on a sensor wafer the same as with an articulated occlusion?
Keywords: Occlusion, T Scan, OccluSense, Sensor. Wafer, Blue Paper.
Teeth consist of vital tissue. They are vascular and contain many touch receptors (1). Teeth micro move upon occlusal contact (2). Marking indicators are made of many materials. The thickness of the indicator determines the size of the contact area (3). False markings lead to the indiscriminate removal of tooth structure. Thin pressure wafers for electronic devices are made of a semi flexible plastic. Figure 1.

In DTR therapy interfering areas of enamel are cited on screen and removed with minimal reduction (4). Mandibular excursions are related to direct tooth contact. Disclusion Time Reduction (DTR) is a form of treatment. Judiciously removing tooth obstructions reduces muscle tension in the facial and masticatory muscles. Relief from pain and disfunction is almost instantaneous (5). Timing is significant. Myofascial pain relief is related to speed of disclusion. Molars should not touch upon disclusion. Many people attest to the curative powers of this treatment (6). The facial muscles relax. Joint pain is reduced. Bruxing and trigeminal neuralgia may be eliminated. Testimonials abound. Much of this treatment is related to the occlusion and bilateral balance. Balancing a bite on a wafer can be achieved but balancing a bite on an articulated dentition may be impossible because of the many different cuspal forms and aberrations. Intra oral visualization of contact markings by a clinician often determines balance. How much sound tooth structure must be removed to achieve a balanced bite? Location and amount of enamel reduction is measured from the wafer and tooth adjustment follows. Speed of disclusion is associated with a balanced bite. An occlusal contact on a wafer differs from tooth to tooth contact.Therapeutic treatment is measured by disclusion time reduction (7). The treatment appears to work but it is not generally accepted by the profession. A balanced bite is a denture term where artificial teeth on both sides of a denture work together. It stabilizes dentures (8). The electronic systems of measurement are precise (9). Is a balanced bite on a wafer the same as a balanced bite on an articulated dentition? Can a clinician balance a bite without a wafer? Do timing and force vectors directly relate to occlusal contact?
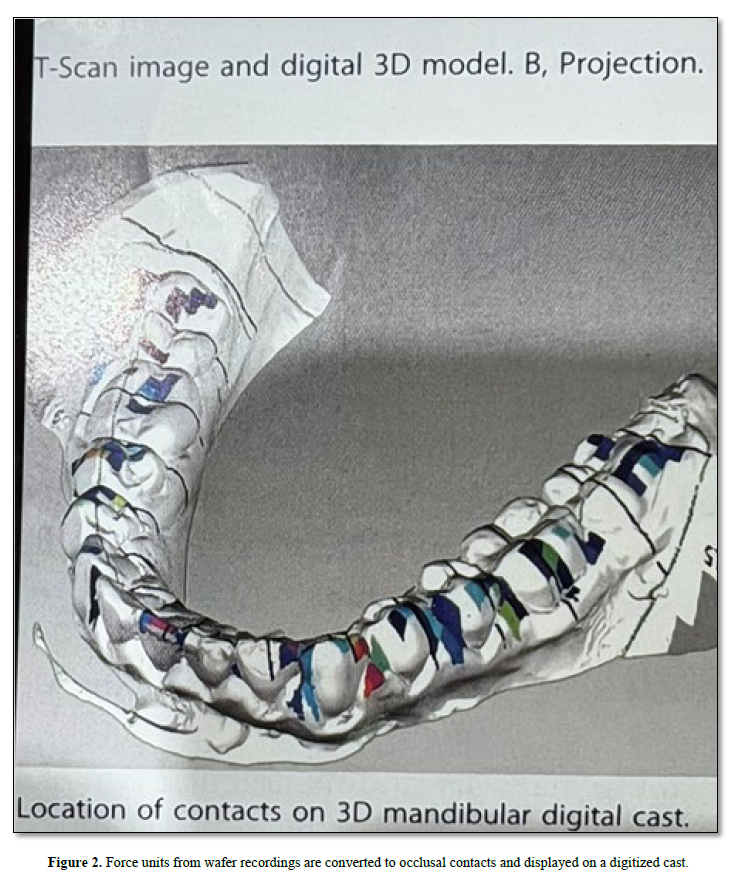
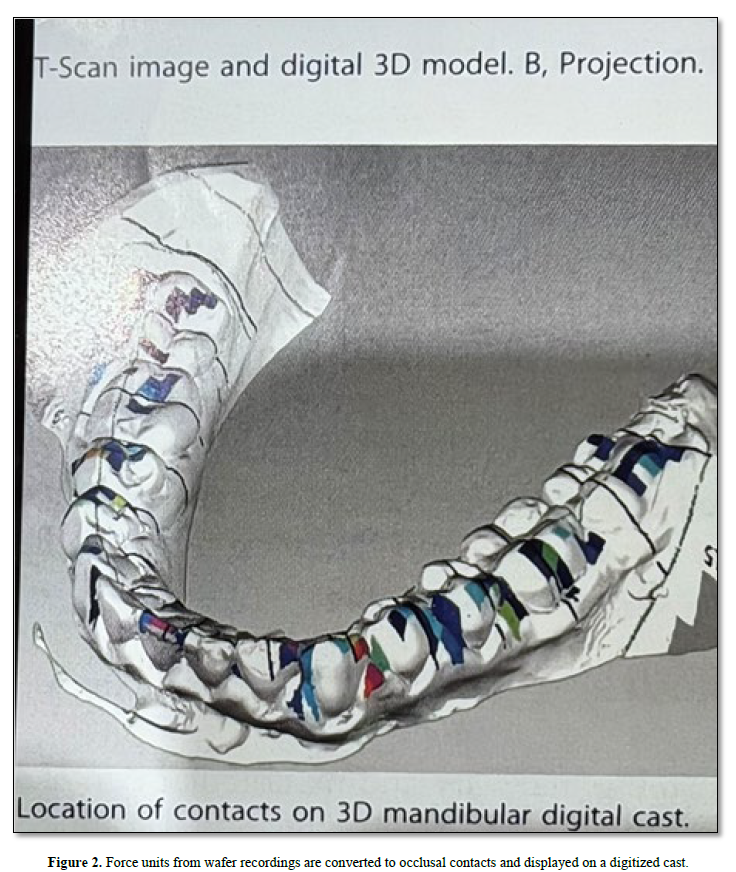
Are the posterior centric stops in function? The consensus is that all teeth should come into contact simultaneously. The force on the right half arch should be equal to the left side. The posterior teeth should have higher force. Opposing contacts should have equal force. In clinical practice a bite does not have to be balanced for it to be functional. Worn teeth are often balanced. A balanced bite can be established on a plastic wafer at an increased vertical dimension but does it correlate with the underlying articulated dentition? The wafer can not record the many aberrations that make up a worn dentition. A clinician can roughly balance an occlusion by minimizing occlusal disharmony. A wafer is not required. All measurements of force or pressure recorded on a wafer are extrapolated to fit their corresponding occlusal surfaces Figure 2.
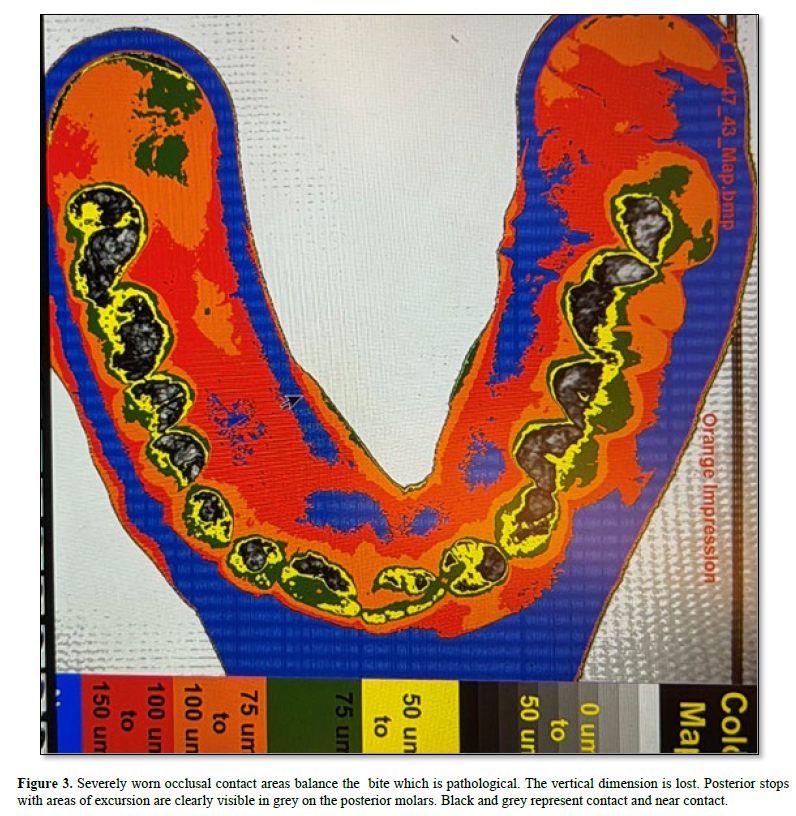
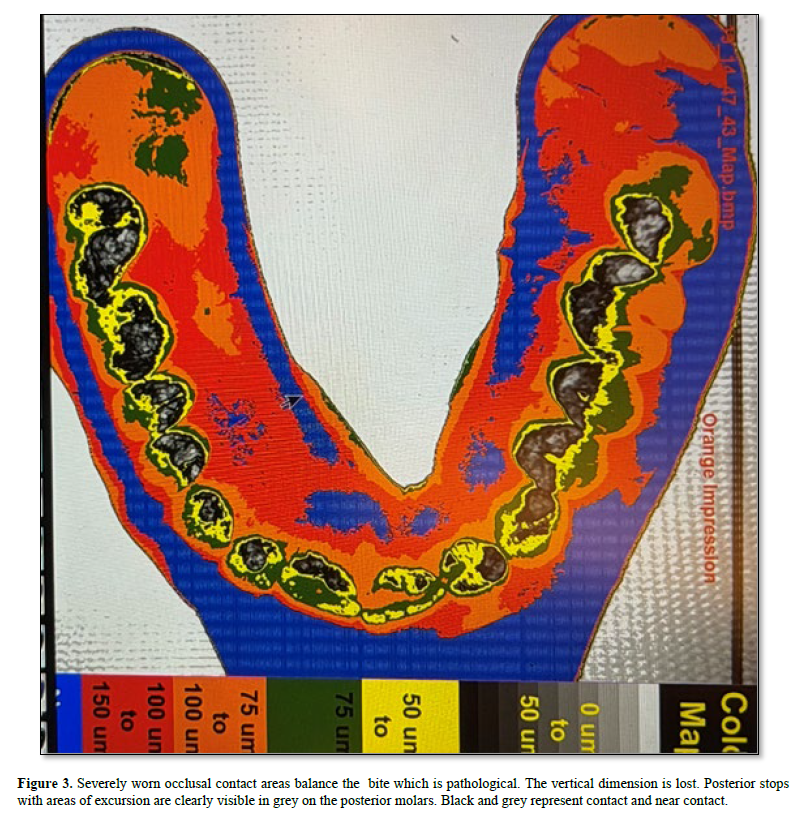
In a simplistic manner clinicians can record the static occlusion along with excursions and intensity of contact by using a light sensitive non set silicone impression material and analyzing movement using image analysis (10) Figure 3. Dental education is remiss in disseminating knowledge of the occlusion. The older rules of occlusion preclude change. Direct occlusal contact has a different meaning than wafer generated contact. Direct contact forms the baseline from which function occurs (11).
The occlusion changes when the vertical dimension is increased by a measuring wafer. The mandible shifts position upon closure. In an existing occlusion each tooth maintains a position with it’s own contact force and movement. Alternative means of measurement should be explored. Sound judgment is required.


No Files Found




Internationally Accepted
Share Your Publication :