
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein* and Carlos E. Sabrosa
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: April 11, 2026 ; Revised: April 15, 2026 ; Accepted: April 18, 2026 ; Available Online: April 20, 2026
Citation: Millstein PL & Sabrosa CE. (2026) Restoring Occlusal Contact on Implant Restorations and Endodontically Treated Teeth. J Oral Health Dent Res, 5(3): 1-3.
Copyrights: ©2026 Millstein PL& Sabrosa CE. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Restoring damaged teeth requires change. The occlusion is difficult to program in weak teeth. Lack of implant mobility is addressed. Designing a new occlusion is advocated.
Keywords: Implant, Root Canal, Restoration, Occlusal Contact.
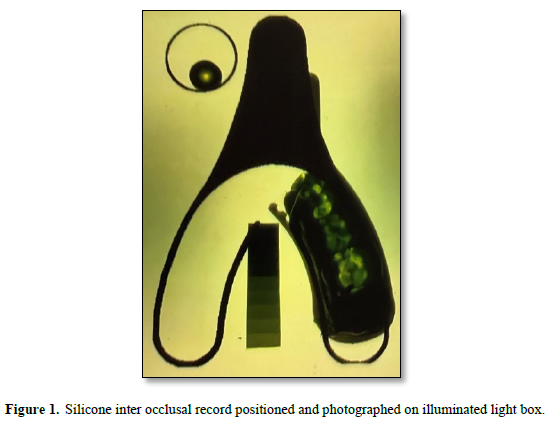
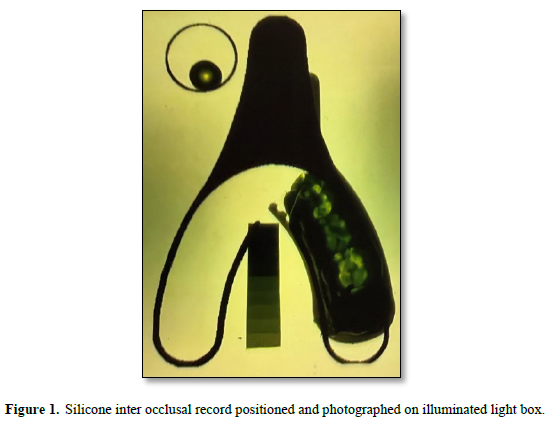
Endodontic therapy is used to treat non vital teeth (1). The internal structure of the tooth is removed and filled with a rubber material. The tooth is weakened and it’s proprioception is no longer acute. The element of touch sensitivity which provides a guide towards tactile contact is altered (2). Endodontists do not restore teeth. It is the clinician’s choice whether or not to rebuild the under structure before the crowning procedure (3). There are many techniques to strengthen the under structure and restore the missing dentin but none is ideal. Proprioception is reduced as is touch sensitivity (4). Endodontists always suggests that completed crown restorations be built slightly out of occlusion or just within touch (5). Proprioception will gently guide the the tooth into a protected occlusal space. Endodontists are untrained in restorative dentistry. The restorative dentist is taught in dental school to make no contact. No clinical professor will elaborate on what light contact or almost contact means. “Go easy” is the catch phrase. Touch does not mean occlusal contact. Intensity of contact can not be measured. Treated teeth maintain their limited mobility but they are weaker. A tooth that is not in occlusal contact can not contribute to a functioning occlusion. There are always slight movements of teeth (6). Auto adjustment is possible. Implant clinicians advocate in lay terms for minimum or light occlusal contact but they can’t explain in didactic terms what they mean. It is a form of double speak where no one can explain what they mean. Physical contact with the opposing dentition is necessary to establish function and the dentist must prescribe the contact placement. Intensity of contact must match that of the other functioning teeth. Contact areas are designed to be minimal but there is actual contact. In clinical terms the occlusal contact of restorations for implants or treated teeth must be assessed intra orally and not with a wand or in the dental laboratory (7). Actual physical contact should occur upon hard closure (Figure 1).
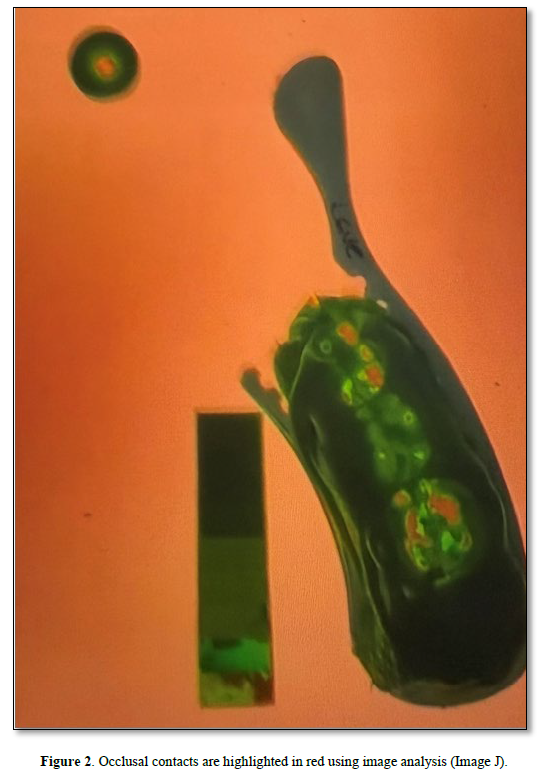
Once the restorations are cemented to place and the occlusal contact areas are adjusted a permanent occlusal record is made (8) Figure 2. The record is used upon yearly examination to assess the occlusion. Adjustments are made according to need. The occlusal restorations for implants and treated teeth are similar but the clinical treatments differ. A treated tooth and an implant restoration must have an occlusal contact in order to function. Slight touch is not sufficient. The implant restoration is an immovable foreign body that will not function unless there is physical contact. The surrounding dentition adjusts to the implant whereas the treated tooth is moveable and adjusts to the surrounding dentition. Both can not sustain occlusal trauma. Vertical force is tolerable but eccentric movements are destructive. Endodontically treated teeth can move but implants are rigid. Contact occlusion differs from “almost” occlusion because physical contact has been made. Physical contact relies upon proprioception and touch sensitivity. Proprioception is a form of spatial recognition. Touch provides a tactile sensation. Proprioception and touch will guide a restoration into a functioning occlusal position. This position will never be ideal but it will be functional because it is in occlusal contact. An under occluded tooth may find an aberrant contact but chance is not a good predictor. In a functioning dentition teeth make small adjustments. It is part of a living system with a rhythm and pattern of its own. Occlusal examinations should be made yearly but clinicians do not take records. No follow up examinations are made. Isn’t it time for change? Occlusion may appear invisible but it is always a determining factor in food selection and oral health.
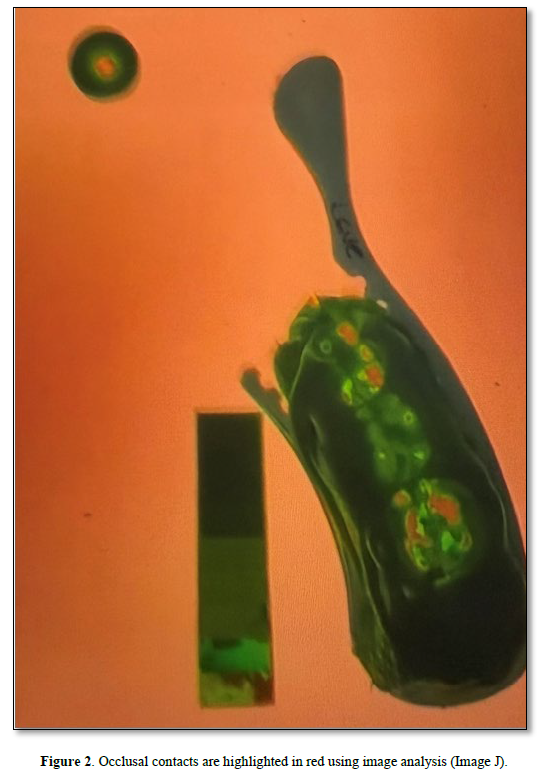
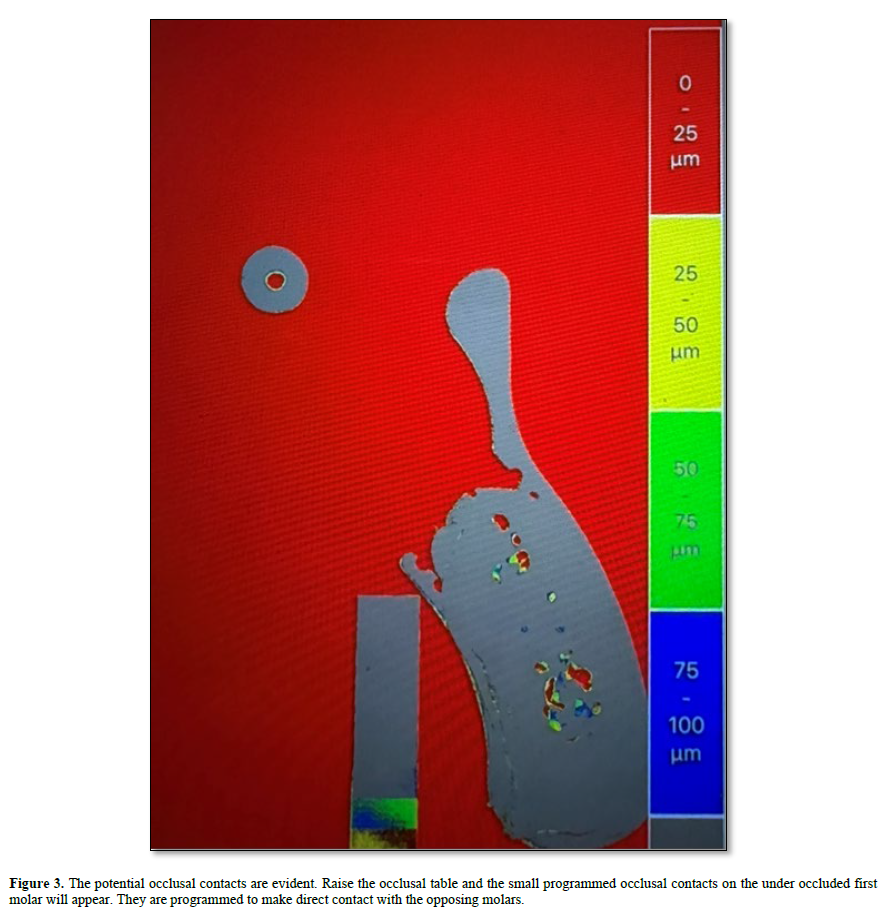
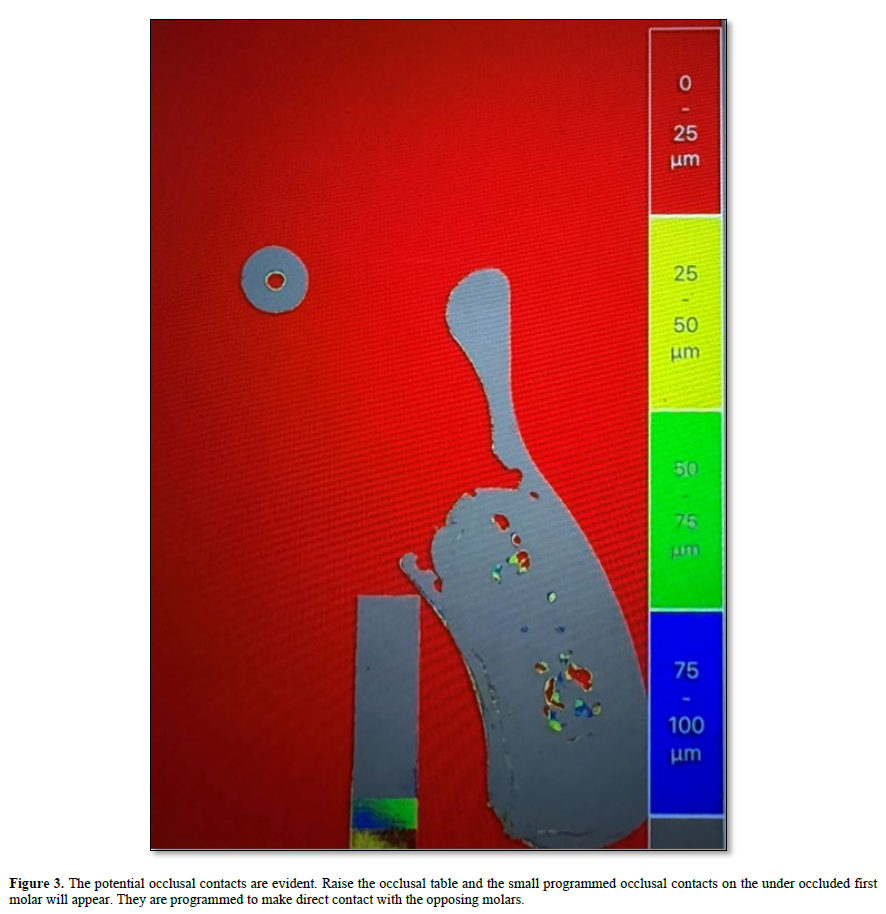
To make a permanent record an inter occlusal impression is made in a triple tray and the impressions is positioned on an illuminated light box (9). A photograph is taken from above and a permanent record is made. The resultant black and white photograph is processed using an image analysis program. Density changes are measured and recorded. A calibrated color scheme is added for visual assessment (10). The color red signifies occlusal contact Figure 3. This recording system is accurate. It was constructed to measure occlusal contact. The making and taking of an accurate impression is the controlling factor. It takes time to learn about the dynamics of occlusion. Practice is suggested.

No Files Found




Internationally Accepted
Share Your Publication :