
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: April 01, 2026 ; Revised: April 05, 2026 ; Accepted: April 08, 2026 ; Available Online: April 10, 2026
Citation: Millstein PL. (2026) Touch Sensitivity and Occlusal Contact in Tooth and Implant Restorations. J Oral Health Dent Res, 5(3): 1-3.
Copyrights: ©2026 Millstein PL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Implant restorations are not touch sensitive. Vital teeth are touch sensitive. Implant restorations differ from vital teeth upon occlusal contact. An alternative occlusal design for implant restorations is suggested.
Keywords: Implant, Occlusion, Touch, Contact, Intensity.
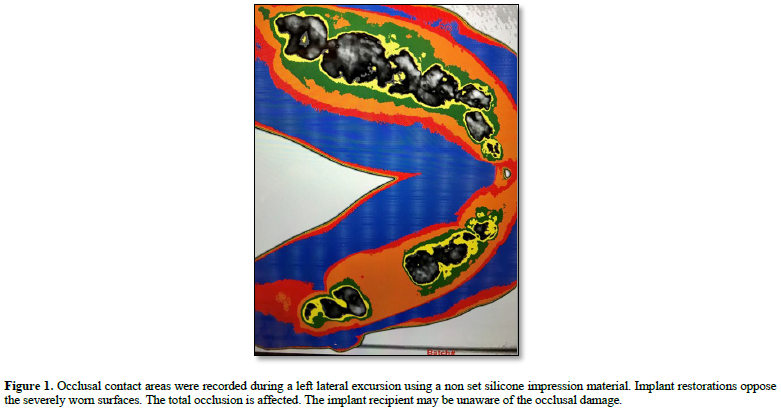
To touch is to contact (1). Touch sensitivity is missing in implant supported restorations (2). Vital teeth in periodontal housings are touch sensitive (3). Touch sensitivity accompanies tooth positioning upon occlusal contact (4). Implant restorations are made from Zirconia which is a ceramic type of metal. It is hard and unyielding (5). Wear in function is minimal. Implants are immovable. They are not touch sensitive. Centric relation is a retruded jaw position which is fixed in space (6). It is a repeatable rotating position which dentists use as a starting point in extensive reconstructions. Most often clinicians do not use the position because it is difficult to find and record. Dentists use a retruded mandibular position which is not repeatable. The position is recorded by making an inter occlusal record. The record is used to position dental casts on an articulator. If the record is incorrect then all of the jaw movements simulated on the articulator will be inaccurate. Upon insertion of a prosthesis the cusp fossa relationships between teeth and implants will clash as a destructive occlusal contact scenario develops. The patient will not sense the difference because implant restorations are not touch sensitive. In a true centric relation oriented case a cusp fossa relationship is developed for each tooth. Opposing cusps fit into matching fossae which are positional stop areas for occlusal contact. The adjacent cusp/fossae areas are used to guide the cusps when they idle and function. There is an established rhythm which is developed for each patient. In the past centric relation cases were made for wax forms which were cast in gold which wears well in function. All teeth were supported by a periodontium which contained many touch receptors. There were no implants . Today zirconia is the preferred material for implant restorations. Implants have little proprioception because they have no touch receptors. When a dentist restores implants the recipient can not sense the intensity of occlusal contact. A balanced occlusion can not be evaluated by the patient (Figure 1).
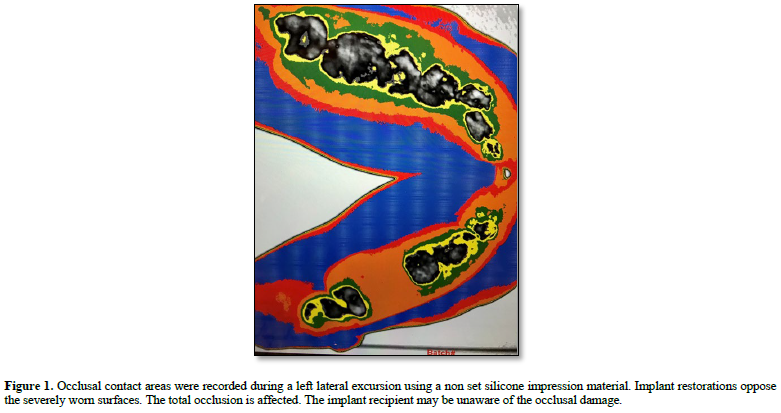
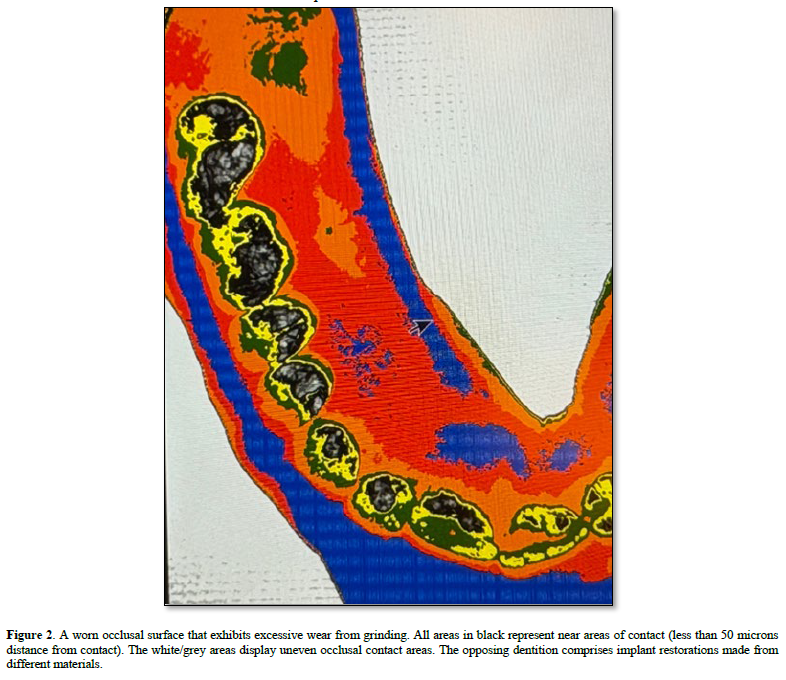
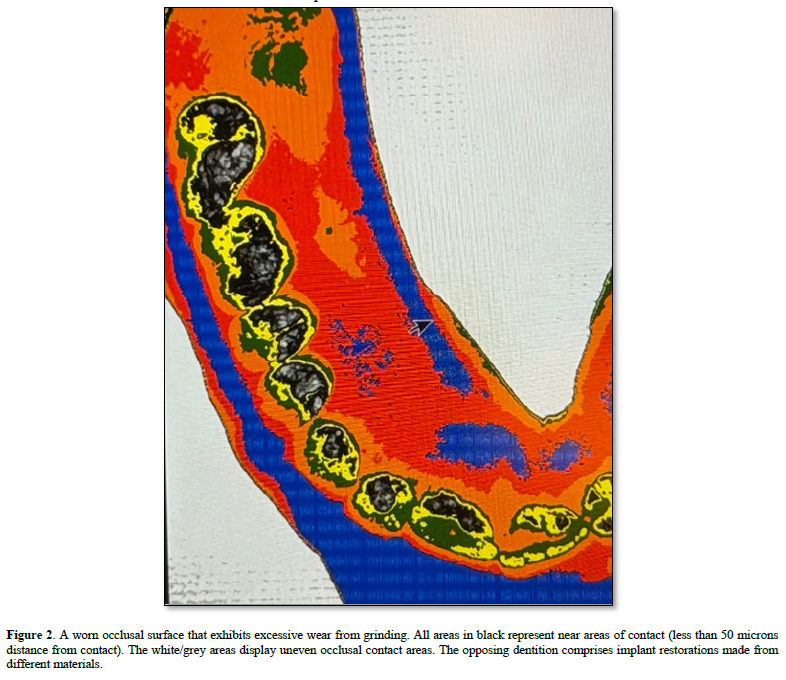
The clinician uses marking papers to measure a balanced bite but his/her measuring system is inadequate (7). The patient determines comfort when touch sensitivity is non existent. Most completed cases survive; some fail. Broken ceramics, reduced bone height, and bacteria infected implant surfaces may occur over time. The working occlusion is not monitored. There are no permanent occlusal contact records. Although dental implant reconstruction is a medical achievement we still use older methods to guide us. Some methods and materials no longer fit modern day protocols. New treatments use new materials. An uneven occlusion with mixed restorations will create occlusal damage Figure 2.
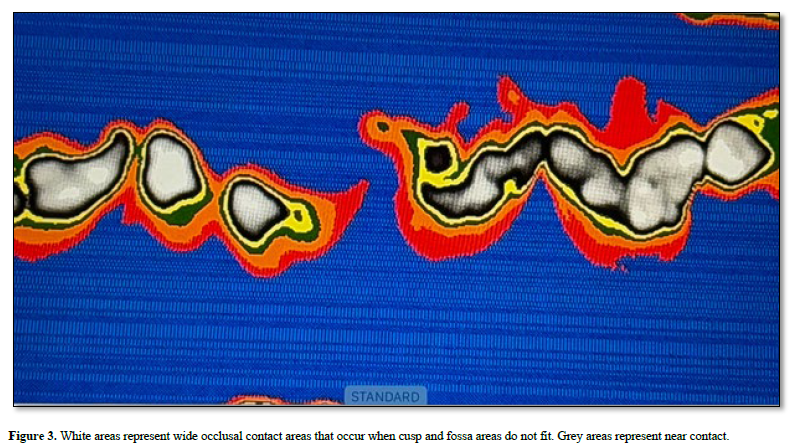
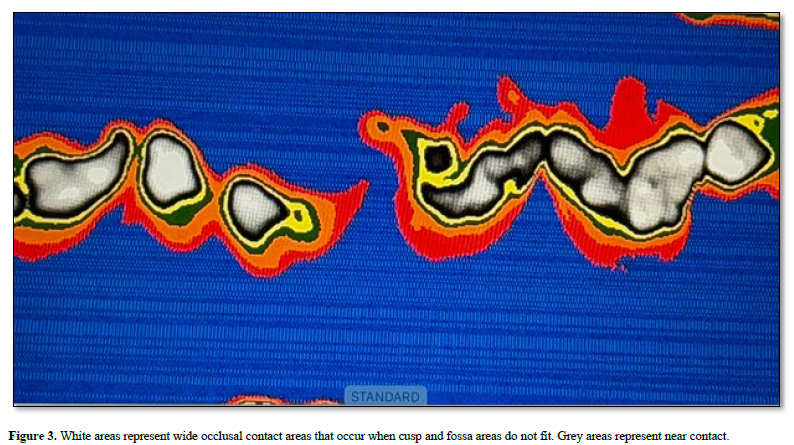
Opposing cusps and fossae should not interlock Figure 3. Occlusal stops should suffice and adjacent occlusal areas should be wide with accompanying shallow slopes or flat surfaces. Older philosophies can be altered to allow for newer techniques and procedures. Occlusal contact records should be saved and periodically reviewed (8). In order to record the occlusion permanently we use a non resistant instant forming silicone impression material. The material is placed onto an adjustable triple tray frame and the patient is asked to bite hard. Rehearsal may be required. The impression is instant. The impression is removed and placed onto an illuminated surface on a digital scanner and a photograph is taken from above (9). An image analysis program is used to evaluate film intensities in the resultant black and white photograph. Color is added for easy viewing. White is contact. Black and grey are near contact areas. In general implant restorations are a success. Occlusal examinations should be made yearly and adjustments made when needed. Prevention is always the goal.

No Files Found




Internationally Accepted
Share Your Publication :