
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Carlos E Sabrosa and Wai Yung
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: March 22, 2026 ; Revised: March 26, 2026 ; Accepted: March 30, 2026 ; Available Online: April 03, 2026
Citation: Millstein PL, Sabrosa CE & Yung W. (2026) Occlusal Damage Can be Recorded. Do We Repair It? J Oral Health Dent Res, 5(3): 1-4.
Copyrights: ©2026 Millstein PL, Sabrosa CE & Yung W. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Diagnosis and or treatment of the occlusion requires an intra oral examination. Permanent Intra oral records are made and examined in an extra oral setting. The rules for occlusion are reviewed. Change is suggested.
Keywords: Occlusion, Contact, Prevention, Wear.
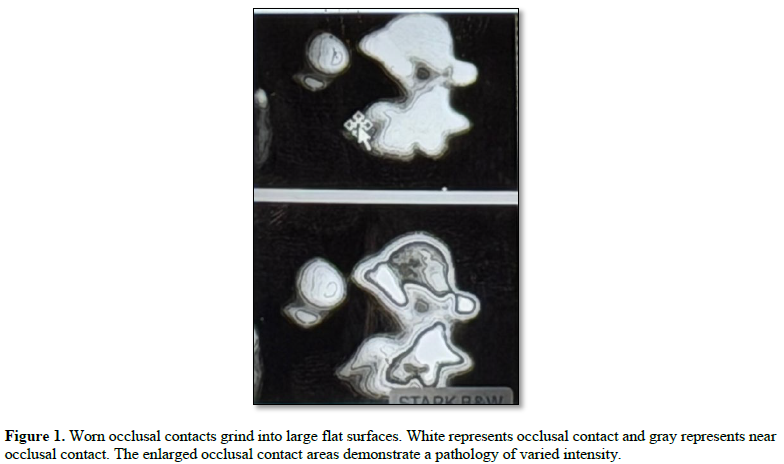
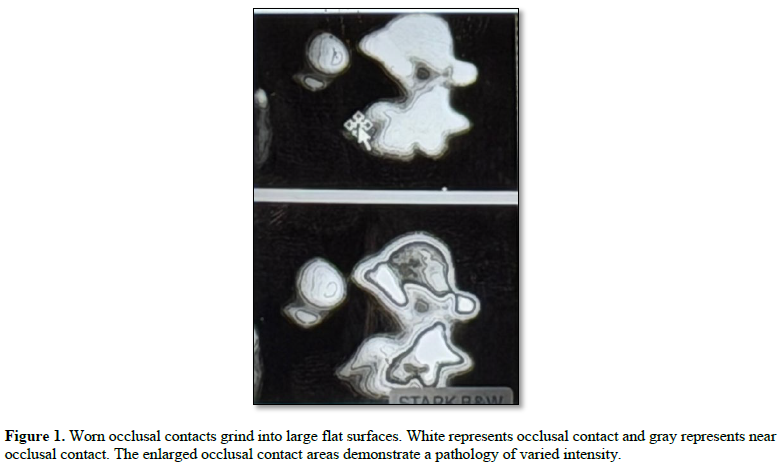
Occlusal wear is damaging (1). Severe wear is pathological. (Figure 1). Clenching breaks teeth and strengthens muscle force. The physical affects of long time wear are clinically visible; the effects on short time wear may be invisible. Sometimes there are no signs of grinding other than the sounds that occurs during sleep.
Grinding and clenching are neurologically driven oral pathologies but where is the starting point when occlusal harmony is lost? (2). Harmony of the occlusion exists when occluding teeth close together without clashing and grinding (3). Occlusal disharmony results when opposing teeth clash and grind and attempt to even out the resulting broken surfaces. When does occlusal disharmony begin? To avert dealing with occlusal problems clinicians refer patients to dental specialists (4). It is no longer the referring clinician’s responsibility. Oftentimes no treatment is considered for older people until heavy restorative work is required (5).
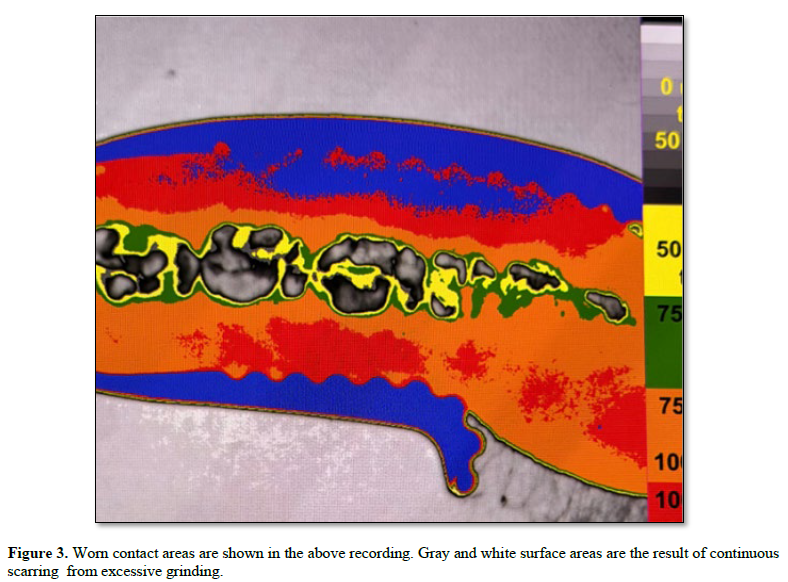
Dental schools teach idealistic dentistry (6). Commercial dental companies teach and sell full mouth implant reconstructions (7). Patients seek out dentists to repair teeth and in all these visits no one closely examines the working occlusion. The patient does not routinely function in a retruded space as often taught by educators but functions in a centralized occlusal contact area which is anterior and superior to the retruded area (8). Where and when does occlusal disharmony become evident? It may be that disharmony is normal and that nature is imperfect. If this premise is plausible then what can a dentist do to minimize structural occlusal damage? A clinician can examine and record a patient’s occlusal profile and review it yearly at routine visits (9) Figure 2.
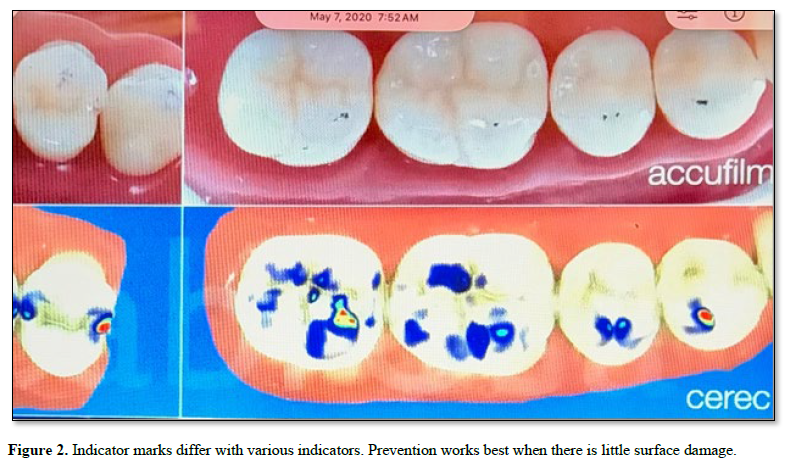
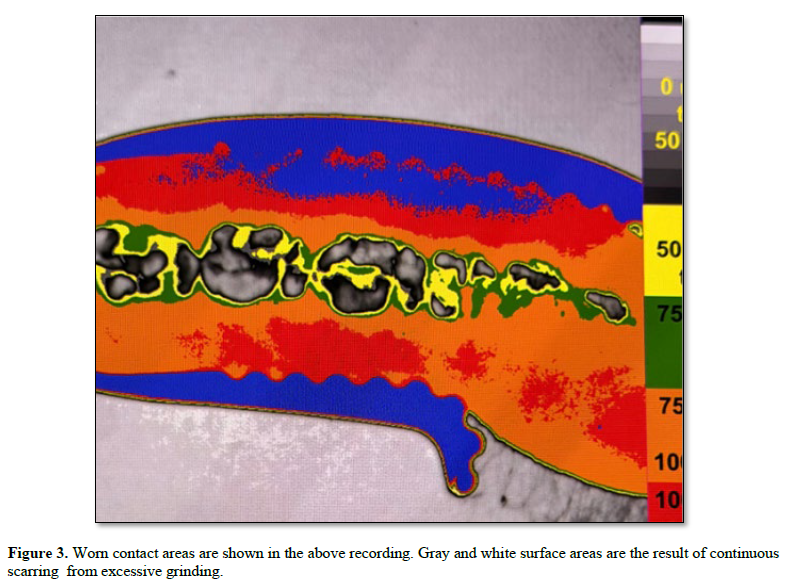
 Health and disease can be evaluated. If dental treatment is instituted and completed it is the practicing clinician who is responsible for the patient’s health. How does a clinician address occlusal health in a patient population? (10). A dental hygienist is a good ambassador.to explain the positive aspects of a sound occlusion. Do current practitioners learn about the science of the occlusion in dental school? Dental training should Include the principles of functional articulation. Do restorative dental teachers reach out to clinical practitioners? The educational system is complex and rarely discussed. How does a clinician know what to do? The biomechanics of tooth function indicate that teeth establish a pattern of wear and that tooth surfaces wear out Figure 3. Theoretically teeth should articulate smoothly with one another but they rarely do. What is the clinician’s responsibility? As children mature the family dentist can monitor their occlusion using the scan and make occlusal adjustments. Slight changes in the cuspal alignment of a tooth can interrupt the intended path to a cusp fossa relationship. If a cusp binds upon occlusal contact a tooth may not fully engage it’s counterpart and the mandible may shift to accommodate the obstruction. Something so remote as cuspal interference can begin the grinding process. If a small occlusal restoration is placed in hyper or hypo occlusion it may not fit readily into the opposing dentition. Small aberrations can cause mandibular dysfunction. An imperfect bite becomes a problem. How can we examine an occlusion intraorally when the view is obstructed? It is not possible. There is no shortage of implant driven restorative work but there are few occlusal recordings that can be used to evaluate the success and failure of the work. The costs for dental restorative work are prohibitive so why do we minimize prevention? If most of the population suffers from dental disease and much of it originates with the occlusion then why don’t we diagnose and treat the occlusion? Examining the occlusion is usually quick and inconclusive. Occlusal malfunction remains hidden and out of sight. A clinician can only examine an occlusion using a specific scan developed to record the elements of occlusal contact and associated closed contact movements. Areas of contact are recorded intra orally and examined extra orally (11). Understanding and studying the patterns of occlusal contact requires careful examination. Clinical training is required. Permanent records are made in a triple tray loaded with impression material. The tray is carefully positioned intra orally and an inter occlusal record is taken. Once made the record is placed on an illuminated light surface located at the base of the scanner. An overhead camera takes a picture and makes a permanent record. An image analysis program (Image J) is used to establish black and grey densities in the photograph and to convert them into a graded calibrated color scheme. Contact and near contact areas are viewed extra orally. White is contact. Black is 50 microns distance from white.
Health and disease can be evaluated. If dental treatment is instituted and completed it is the practicing clinician who is responsible for the patient’s health. How does a clinician address occlusal health in a patient population? (10). A dental hygienist is a good ambassador.to explain the positive aspects of a sound occlusion. Do current practitioners learn about the science of the occlusion in dental school? Dental training should Include the principles of functional articulation. Do restorative dental teachers reach out to clinical practitioners? The educational system is complex and rarely discussed. How does a clinician know what to do? The biomechanics of tooth function indicate that teeth establish a pattern of wear and that tooth surfaces wear out Figure 3. Theoretically teeth should articulate smoothly with one another but they rarely do. What is the clinician’s responsibility? As children mature the family dentist can monitor their occlusion using the scan and make occlusal adjustments. Slight changes in the cuspal alignment of a tooth can interrupt the intended path to a cusp fossa relationship. If a cusp binds upon occlusal contact a tooth may not fully engage it’s counterpart and the mandible may shift to accommodate the obstruction. Something so remote as cuspal interference can begin the grinding process. If a small occlusal restoration is placed in hyper or hypo occlusion it may not fit readily into the opposing dentition. Small aberrations can cause mandibular dysfunction. An imperfect bite becomes a problem. How can we examine an occlusion intraorally when the view is obstructed? It is not possible. There is no shortage of implant driven restorative work but there are few occlusal recordings that can be used to evaluate the success and failure of the work. The costs for dental restorative work are prohibitive so why do we minimize prevention? If most of the population suffers from dental disease and much of it originates with the occlusion then why don’t we diagnose and treat the occlusion? Examining the occlusion is usually quick and inconclusive. Occlusal malfunction remains hidden and out of sight. A clinician can only examine an occlusion using a specific scan developed to record the elements of occlusal contact and associated closed contact movements. Areas of contact are recorded intra orally and examined extra orally (11). Understanding and studying the patterns of occlusal contact requires careful examination. Clinical training is required. Permanent records are made in a triple tray loaded with impression material. The tray is carefully positioned intra orally and an inter occlusal record is taken. Once made the record is placed on an illuminated light surface located at the base of the scanner. An overhead camera takes a picture and makes a permanent record. An image analysis program (Image J) is used to establish black and grey densities in the photograph and to convert them into a graded calibrated color scheme. Contact and near contact areas are viewed extra orally. White is contact. Black is 50 microns distance from white.
All measurements are in (mm) microns. All other color variations represent near and far occlusal contacts. Learning about the occlusion requires time and dedication. It is the vehicle of occlusal function. Occlusal contact areas are used to stabilize mandibular positions. Comprehensive oral examinations include occlusal contact evaluations. Dental health maintenance requires taking, making and storing occlusal records which are routinely examined. Without clinical participation occlusal health will remain an enigma. It is no mystery. Food choice and good health depend on a sound occlusion.

No Files Found




Internationally Accepted
Share Your Publication :