
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: March 17, 2026 ; Revised: March 19, 2026 ; Accepted: March 20, 2026 ; Available Online: March 25, 2026
Citation: Millstein PL. (2026) Occlusaline: Therapeutic Bite Alignment. J Oral Health Dent Res, 5(3): 1-4.
Copyrights: ©2026 Millstein PL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Therapeutic bite guards should be prescribed to prevent occlusal trauma. They may also be used to reduce dysfunctional mandibular movement. Clinical studies are suggested.
Keywords: Occlusion, Trauma, Dysfunction, Prevention
Occlusion means to close (1). The jaws should align comfortably with one another but they rarely do. It is assumed that opposing occlusal contact areas will self adjust by grinding into one another (2). Years later the dentist suggests an occlusal guard (3). The patient wears it down until it breaks (4). There is no occlusal profile for review. Not much clinical acumen is spent with the design and delivery of occlusal appliances. Dentists do not design bite guards as therapeutic splints. They are used as “bite stops” A dentist could treat the occlusion by designing and making personalized bite appliances. Every patient has a specific bite pattern so they require specific bite surfaces.
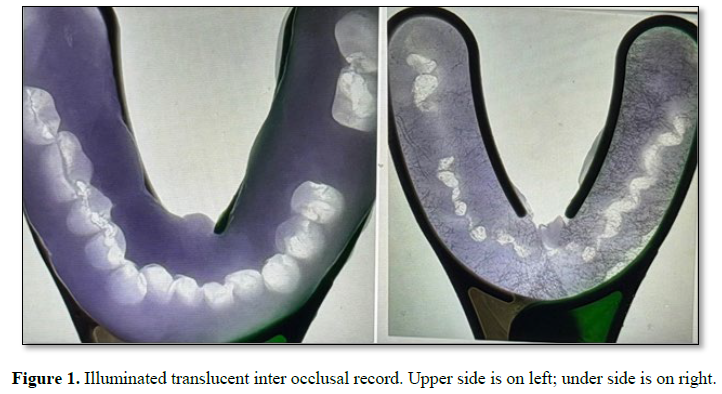
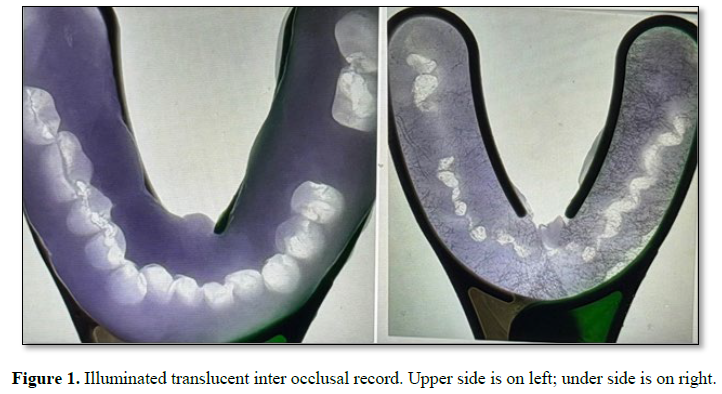
All fingerprints differ and no two bites are alike so why make all bite guards alike? (5). Occlusal profiles can remain the same or improve with clinical intervention. A clinician needs an overall picture of the occlusion to plan for occlusal change. This includes a static and functional bite (6). Bite recordings are made, illuminated, photographed and projected onto a computer screen for study (Figure 1).
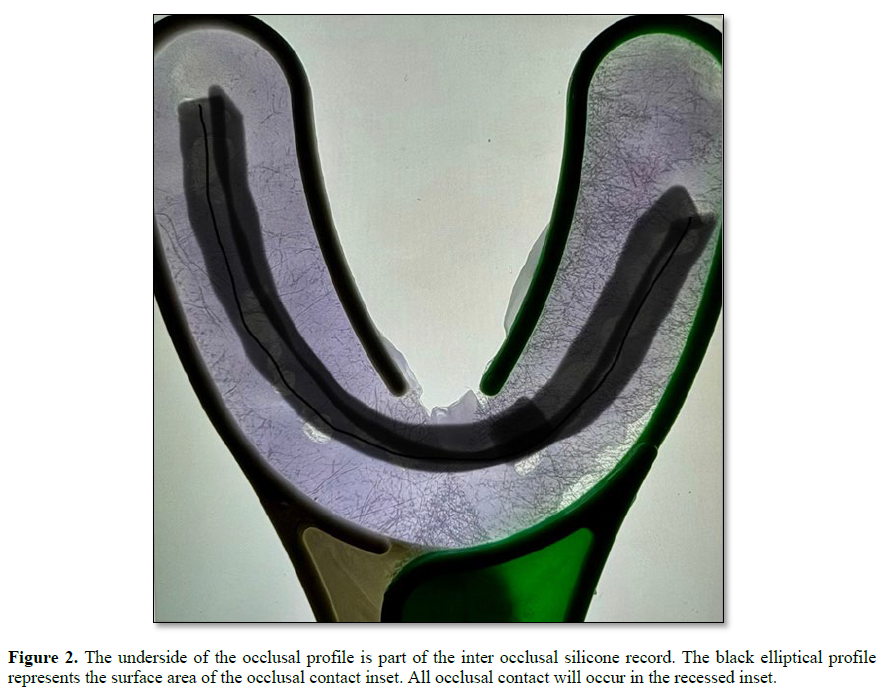
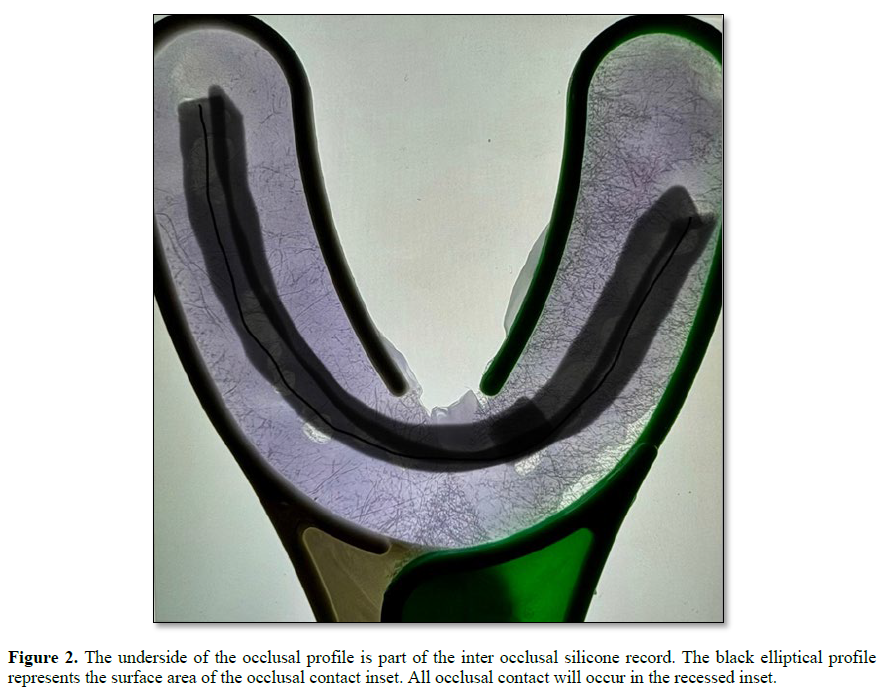
The clinician assesses the occlusion. How severe is the bite problem? How many teeth remain? How old and infirm is the patient? What is the endpoint of treatment? Will temporary treatment suffice? (7). Companies sell “do it yourself” bite appliances. Dentists prescribe bite guards. There are no occlusal records. How can clinicians realign occlusal positions without keeping occlusal records? A bite appliance is a therapeutic device. It is used to reposition and stabilize mandibular jaw positions. A clinician can design and manufacture personalized occlusal devices. Computer programs can be used to process and print designs onto surfaces of bite appliances. In order to make an occlusal device a clinician requires a basic occlusal profile. The profile can be studied and used to prescribe a therapeutic splint (Figure 2).
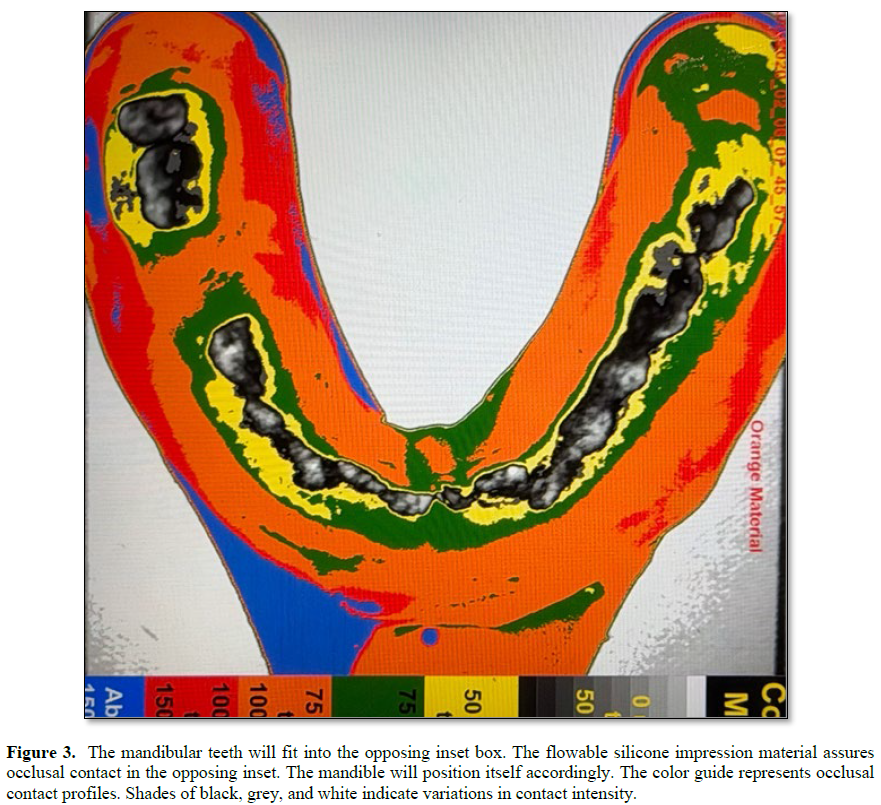
Bite splints wear out. They should be changed periodically with the patient’s understanding that splints are personalized therapeutic appliances. It is also a good idea for a clinician to stabilize a physical bite before performing extensive restorative work. Prescription bite guards may not be popular but designing a therapeutic occlusion is worth considering. If a patient can not adjust to a personalized contact surface then remove the appliance. The treatment is reversible. An individualized occlusal contact profile is fit into the occluding surface of a processed maxillary bite splint. The opposing mandibular dentition is then fit into the occlusal inset on the splint. The recorded mandibular occlusal profile is positioned into the inset on the occlusal surface of the maxillary appliance. It is like a lock and key configuration. The mandibular dentition fits into the matching maxillary inset. Occlusal contacts provide areas for mandibular stability (Figure 3).
The occlusal profile box is deep enough and wide enough for limited mandibular excursions. A good fit of the mandibular dentition into the opposing inset requires occlusal adjustments. Some clinical cases may be too extreme for mandibular stabilization. A dentition will easily fit into the opposing individualized inset. The purpose of the inset is to stabilize jaw movement and to reposition the jaw. The dentist makes required adjustments over time. If upon usage excess wear takes place a malleable safe metal insert can be cut, fit and inserted into the box. Mandibular fit is assured because the occlusal profile that is visible on the underside of the inter occlusal record fits the upper side (Figiure 2).
The fit of the opposing arches to one another is assured. A personalized occlusal profile has been established. The appliance is printed. The procedure can also be done manually. To assess progress compare the inter maxillary occlusal contact areas from before and after treatment and assess mandibular stability. Success or failure is subjective but occlusal contact measurements are objective. Occlusal diseases such as bruxism and severe clenching are neurologically driven but their occlusal pathology is clearly visible. The goal of wearing occlusal devices is to control mandibular dysfunction.
If we can modify the bite using a removable appliance then we can minimize occlusal damage. Programming in office printed appliances is a good place to start. Treatment can be affordable. Clinical oversight is part of the treatment. Comparing permanent occlusal records over time is of clinical value. We as clinicians have two choices: Watch and wait or do something.
This is the clinicians’ choice. Treatment begins with recording occlusal contact. Recordings are made permanent and are easy to store. We use a non set silicone impression material to make static and functional records (8). The impression material is placed on one side of a fitted triple tray impression carrier and the patient is asked to bite hard. The impression is illuminated and photographed. The record is now permanent. The procedure is repeated but the patient is now asked to bite hard and to “grind around” in a closed position The illuminated impression is photographed from above. Permanent static and functional occlusal records are made and saved for review. Total time for impression making and photography is two minutes for each photograph. Total cost is minimal. The photograph is analyzed using an imaging program (Image J). Resulting black and white images are converted to color for easy viewing (Figure 3).
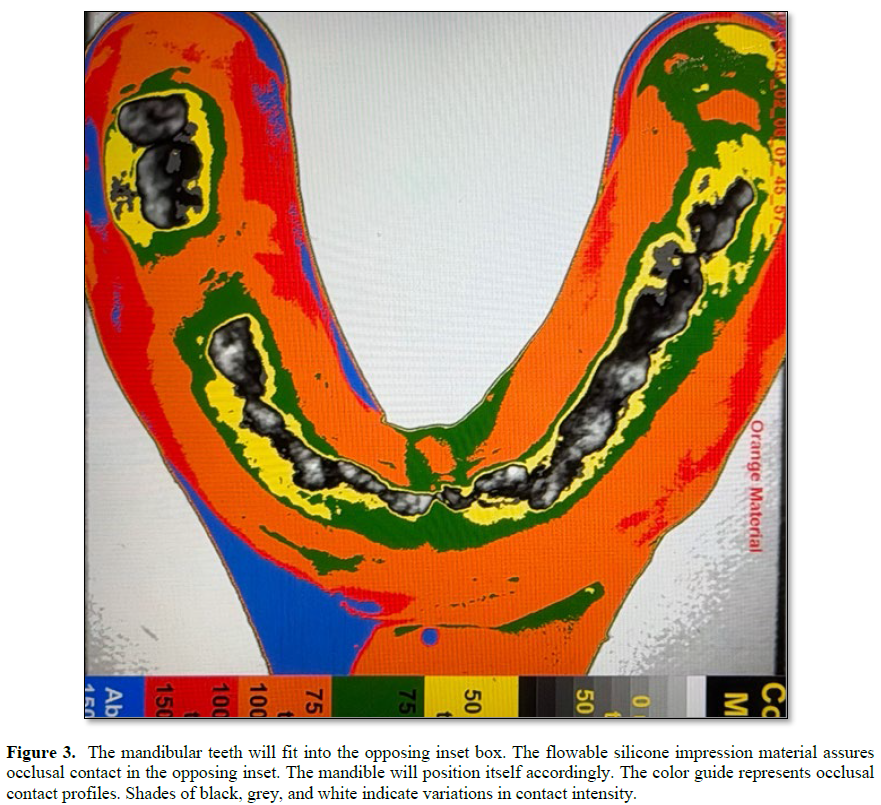
The colors represent graded areas of occlusal contact and non contact. The Inset in the appliance is one millimeter deep. The periphery is established by the recorded bite area on the underside of the inter occlusal record (Figure 2). The total thickness of the bite guard is three millimeters. The imaging system is used to record the occlusal contact at the time of appliance delivery and during and after therapy. Success and failure are permanently recorded.

No Files Found




Internationally Accepted
Share Your Publication :