
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Carlos E Sabrosa and Wai Yung
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: March 01, 2026 ; Revised: March 05, 2026 ; Accepted: March 08, 2026 ; Available Online: March 11, 2026
Citation: Millstein PL, Sabrosa CE & Yung W. (2026) Baseline Occlusion: A Profile. J Oral Health Dent Res, 5(2): 1-3.
Copyrights: ©2026 Millstein PL, Sabrosa CE & Yung W. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This paper asks why dentists don’t record an occlusal contact baseline at the time of dental examination and refer to it at subsequent visits? Periodontal pockets are measured and caries is assessed but occlusal contact is not discussed.
Words: Occlusion, Baseline, Contact, Record
A physician records blood pressure using a precise electronic measuring system. He/she has a baseline to compare past to present readings and to prescribe medication should it be needed. Using image analysis Orthopedists assess healing by measuring bone density changes on radiographs (1) Dentists don’t routinely record the occlusion or save the findings. They mark and remark occlusal contacts using rudimentary marking devices (2). Impression materials have changed over the past century yet there is still no standard means to record the occlusion and it’s various movements (3). We can scan and digitize the occlusion but volitionally holding the teeth together to record an occlusal position with a digitizing wand may not be repeatable or accurate. Intensity of contact is not assessed even though it is a significant factor in implant function (4). We can not effectively record occlusal contact movement (5).Technology has forced dentistry into a new age but dental occlusion remains in the past (6). We still do not record the working occlusion nor do we create a baseline for comparison. We have the tools and materials but occlusal function has not been recorded. Dental school education still relies on outdated models that were created in the early part of the last century (7). Idealized dental casts that are used to teach idealized occlusal schemes do not address clinical demands. Gnathology and centric relation are a significant factor in full mouth reconstruction but they do not fit into general dental practice (8). Centric occlusion and it’s various positions are what clinicians understand. Teaching idealized occlusal schemes does not help students or practitioners because they can never clinically adjust an occlusion to an idealized position. Such a position only exists in dental anatomy texts. Clinical attempts to achieve unattainable goals leads to aborted ends. The articulations do not fit the patient. The teeth do not work in harmony. The patient adjusts? Alternative means of electronic recording of the occlusion were introduced last century but they record force by extrapolating force information from a plastic wafer (9). The system like all occlusal measuring systems is untested. Are the readings accurate? There is no way to know because there are no official standards. We need a standard.by which to compare different methods of occlusal measurement. Materials and methods should be evaluated. Our current system of measurement includes blue paper, red paper, shim stock and type writer ribbon. Clinical accuracy is evaluated in the dental office. There is no standard nor is there any way for making a permanent record of the occlusion. Since a balanced bite is an essential element of the occlusion measuring both sides of the arch is required. The occlusion is generally ignored. It is not taught effectively in the dental schools. The ramifications are evident. With so much progress in the field of restorative dentistry the importance of the occlusion has been neglected. Measuring blood pressure was elusive until a suitable and reliable measuring device was instituted. The occlusion too is elusive but finding a way to permanently record it does not exist. Dental treatment is planned using dental casts but the area, size and intensity of occlusal contacts is not included. The only way to make such assessments is by taking intra oral impressions and examining them extra orally. Using rigid casts will not suffice. Every tooth articulates at a different intensity so when assessing tooth contact specific indicators might be selected. By placing occlusal contact images on a computer screen the clinician can best see and evaluate the occlusion (10). The scan system can be used to evaluate health as well as disease and should be used at routine dental visits. Occlusal disease begins small and at any age. Prevention Is the key to oral health but if you can not see you can not diagnose.
Occlusal examination should occur alongside caries and periodontal evaluation. Permanent records should be made for reference. Occlusal health can be achieved. The challenge lies with the clinician.
We use a simple inexpensive measuring system to record and store information.
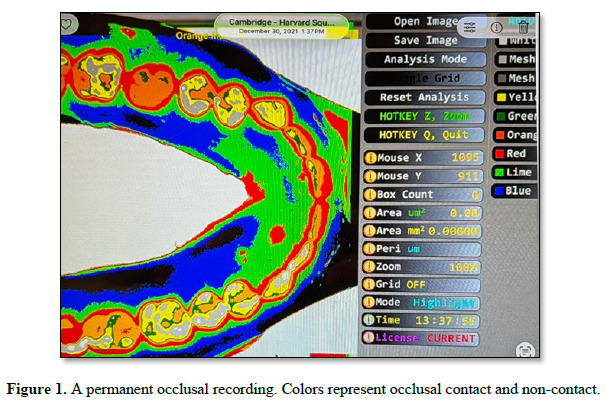
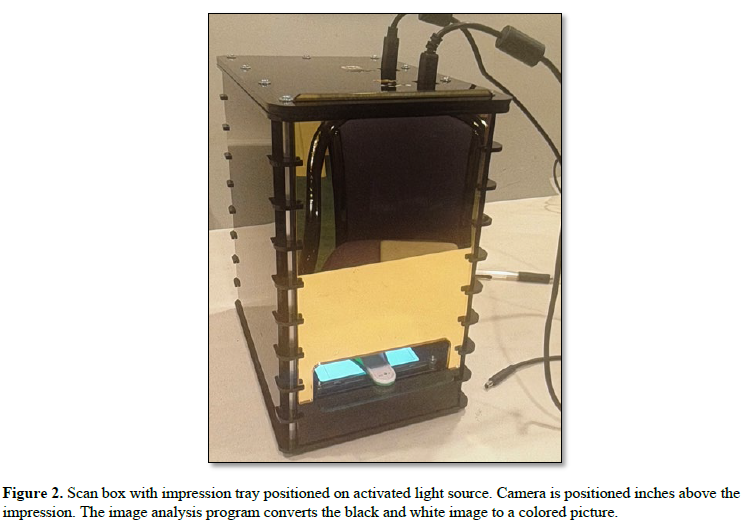
A non-polymerizing polysiloxane impression material is used to impress contact and non-contact areas and to record inter contact movements (11). The material offers little resistance to closure and is light transmissible. The occlusal contact areas are fixed and read immediately using imaging software. A permanent record is made Figure 1.
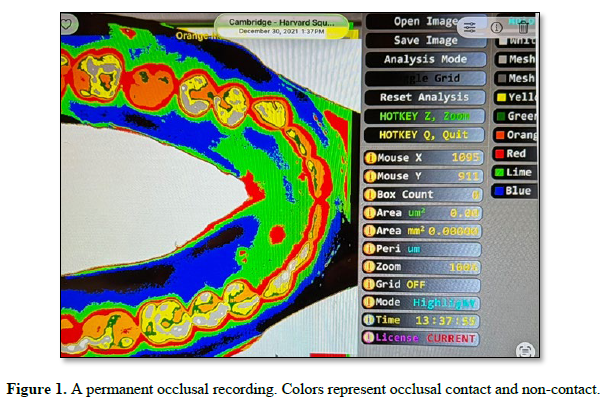
The impression material is reusable with the same patient. The procedure involves using a reference grid to establish the relationship between transmitted light and impression thickness. The impression is made using a triple tray which is positioned on a light box and is photographed from a distance above Figure 2.
 The information is analyzed using an image analysis program (Image J). A grey scale image is colorized using the grid. The images are projected on a computer screen. Study and planning is now possible. Permanent setting silicone impression materials can be used however they are more expensive and do not record movement. All of the information presented here is a product of in office clinical research and all information is original.
The information is analyzed using an image analysis program (Image J). A grey scale image is colorized using the grid. The images are projected on a computer screen. Study and planning is now possible. Permanent setting silicone impression materials can be used however they are more expensive and do not record movement. All of the information presented here is a product of in office clinical research and all information is original.

No Files Found




Internationally Accepted
Share Your Publication :