
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Wai Yung and Carlos E Sabrosa
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: February 16, 2026 ; Revised: February 18, 2026 ; Accepted: February 20, 2026 ; Available Online: February 23, 2026
Citation: Millstein PL, Yung W & Sabrosa CE. (2026) Posterior Bite Collapse. J Oral Health Dent Res, 5(2): 1-3.
Copyrights: ©2026 Millstein PL, Yung W & Sabrosa CE. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Posterior bite collapse is a common oral malady. It goes unrecognized until it cannot be reversed. A means for clinical examination and control of the chronic pathology is suggested
Keywords: Posterior bite, Anterior bite, Occlusal contact, Baseline record
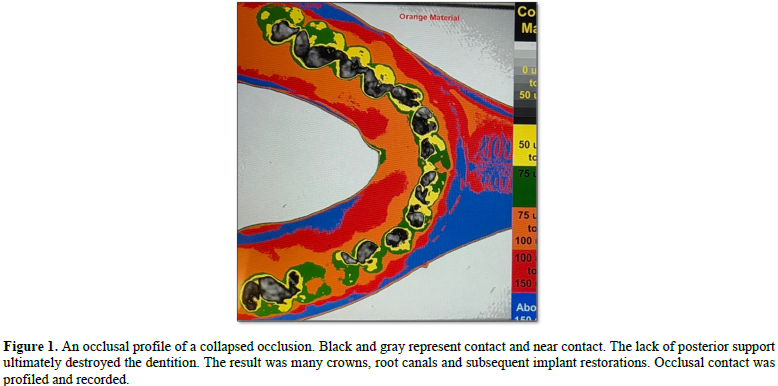
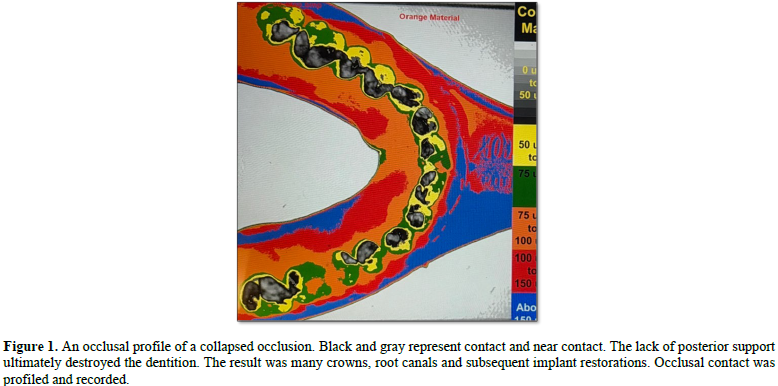
Holding cusps make contact with opposing fossae to hold the teeth and jaw in place. They are rare. Support cusps support their antagonists (1). They are common. Non support cusps make no occlusal contact. They are abundant. Posterior bite collapse is a very common disease which is accompanied by a slow downward forward growth of the mandible (2). Without cuspal support the mandible can not maintain a stable position. Most anyone who visits a dentist for restorative work suffers from it. It is silent but eventually becomes self evident when teeth break or pain ensues. Orthopedic surgeons do not repair a fibula without multiple radiographs using image analysis to analyze bone density (3). Healing is measured by change in density. We as clinicians use “blue paper” to assess the occlusion (4). Intensity of contact can not be assessed, (5). Shape, size, and location of occlusal contacts can not be measured. Infra occlusion is not recorded.There is no permanent record made which reflects our functioning occlusion. Our system of recording the occlusion is incomplete. A unique way to record the occlusion is by making an occlusal recording of the bite in full closure (6). A triple tray is loaded on one side with silicone impression material. The patient bites hard. Upon set the tray is placed on an illuminated (dc) light box which is positioned six inches below a fixed camera which is connected to an image analysis program(ImageJ). Images are digitized and converted to color and displayed on a computer screen (Figure 1).
Variations in occlusal contact and non contact areas are measured and recorded. The information is stored. A baseline has been created that can be used to evaluate occlusal health. Modern day gold casting was patented in 1912 (Taggart). Porcelain to metal crowns were introduced in 1962 (Weinstein). Zirconia crowns are the most popular crowns in use today. (Glidewell). They are strong, wear little and are comparatively inexpensive. Commercial zirconia crowns are made with a large cement space so that fit will never be a problem (7). A crown may shift position upon cementation because of the enlarged cement space. The occlusion is often made just short of contact. The patient and dentist are both happy but where does the occlusion fit in? Restorations using various procedures and materials are used to restore the occlusion but in general they do not make occlusal contact. Posterior bite collapse is an oral disease that persists in spite of advanced technology (Figure 2).

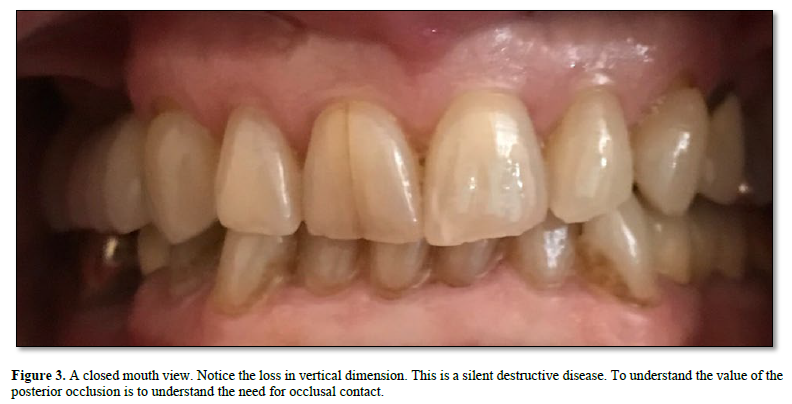
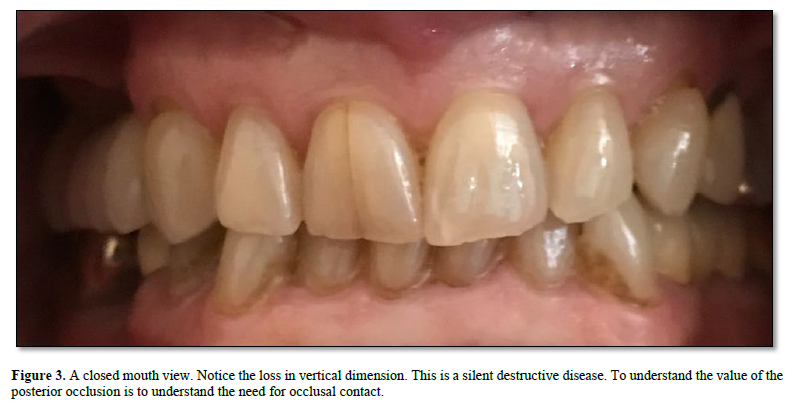
It is the clinicians and the technicians and not the technology that is at fault. Without looking at the incipient occlusal problems and treating them accordingly posterior bite collapse will continue (Figure 3).
The occlusion cannot be fully examined without a full arch occlusal profile that is made intra orally and viewed extra orally. (8). It becomes a much-needed baseline. Full mouth implant restorations may look good upon delivery but their occlusion is not measured or recorded. Preventive occlusal treatment is longer lasting and much less destructive than full mouth reconstruction. If you cannot see the occlusion, you cannot fully diagnose and treat it. The rest is self-evident.


No Files Found




Internationally Accepted
Share Your Publication :